New Publication from GW Researchers Highlights Link Between Aspirin use and Decreased COVID-19 Severity in Hospitalized Patients
A recent clinical research report led by Jonathan H. Chow, Assistant Professor of Anesthesiology and Critical Care Medicine at the George Washington University, found that the use of aspirin may be associated with improved outcomes for hospitalized COVID-19 patients. The study entitled Aspirin Use Is Associated With Decreased Mechanical Ventilation, Intensive Care Unit Admission, and In-Hospital Mortality in Hospitalized Patients With Coronavirus Disease 2019 was published in the journal Anesthesia & Analgesia tracked 412 adult patients with COVID-19 and suggests that aspirin may provide lung-protective effects that help reduce the need for mechanical ventilation and ICU admissions. The article was featured in a recent news release from the American Association for the Advancement of Science. A randomized control trial is now needed to assess whether there is a causal relationship between aspirin use and a reduction in lung injury among COVID-19 patents.
Cells in brain organoids made from human stem cells can mature to resemble those of a postnatal brain. S. Pasca - Pasca Laboratory/Stanford University.
In a recent article in the American Journal of Bioethics, Henry T. Greely explores the ethical implications of improved human brain models used in research. Mr. Greely identifies challenges with using human and animal subjects for brain research, and explores the ethics of improved simulacrum of living brains created and used in research:
The dilemma? When we avoid unethical research by making living models of human brains, we may make our models so good that they themselves deserve some of the kinds of ethical and legal respect that have hindered brain research in human beings. If it looks like a human brain and acts like a human brain, at what point do we have to treat it like a human brain—or a human being?
Mr Greely identifies four types of human brain surrogates: genetically edited non-human animals, human/non-human brain chimeras, human neural organoids, and living ex vivo brain tissues. For each surrogate type, Mr. Greely describes the science behind the surrogates and current directions of the research. Mr. Greely also discusses potential problems with each of these surrogates including welfare of the surrogates, consent and welfare of the “human parts” of the surrogates, possible non-research implications of the research, possible non-research uses of the surrogates, humanization of non-humans, and the rights of the surrogates.
Drawing on references from both science and science fiction to illustrate both technologies and applications, the article is a fascinating read!
If you're interested in reading more about genetics, check out GW's Genetics Journal Club led by Dr. Chuck Macri.
In an effort to remain accountable to communities who have been negatively impacted by past and present medical injustices, the staff at Himmelfarb Library is committed to the work of maintaining an anti-discriminatory practice. We will uplift and highlight diverse stories throughout the year, and not shy away from difficult conversations necessary for health sciences education. To help fulfill this mission, this week’s blog post will feature a conversation with Dr. Raymond Pla, MD.
Dr. Raymond Pla
Dr. Raymond Pla is an Assistant Professor of Anesthesiology and Critical Care Medicine at GW. He received his BS from Emory, then went on to Meharry Medical School, one of four HBCU medical schools, for his MD. I was honored to speak with Dr. Pla about his path to the health sciences, the work he does as a Professor at GW, and his people-first approach to advocacy, particularly when speaking with communities of color.
Dr. Pla did not always intend to go into medicine, he “had the same dreams that you commonly encounter when you're talking to young boys.” Even when he first started his BS program in Biology at Emory, he did not intend to go into medicine, though it was an option. The summer after his Junior year, however, that changed. Over the summer, he had the opportunity to shadow Dr. Clive Callendar at Howard University, going on rounds, in the ICU, and even observing in the OR. A titan in the field of transplantation, especially kidney and liver, Dr. Callendar’s high expectations of his residents, interns, and even the young Dr. Pla set a high standard for medical education. What most fascinated Dr. Pla during his time in the OR was “that person up at the head of the table, on the other side of what we call the ether screen… the anesthesiologist.” Eventually, Dr. Pla started observing with the anesthesiologist, learning what their role was in transplant surgery. Seeing the patients the next day, looking at their labs and seeing the changes in their clinical course overnight, was the second most impactful part of the experience. When Dr. Pla started at Meharry, his classmates reported he already had every intention of going into anesthesiology.
The impact Dr. Callendar had on Dr. Pla is evident, as is Dr. Pla’s desire to pay that influence forward in his practice and teaching. He described what he considers the two most important things doctors, especially those in academic medicine, do. First, “we care.” It is not just about an accurate diagnosis or a successful course of treatment. The foundation of those things is caring - thinking about a patient’s condition in the shower or on a jog or sitting in traffic, jotting down a realization and following up on it the next day, revising the patient’s treatment plan based on these considerations and reflections. And sticking with patients, following them throughout their course of treatment. Dr. Pla described the importance of making time for patients as a part of this, saying “We’ll sit and listen when we don’t have time. When we’re busy, we have someplace else that we need to be. We will redefine where we need to be and where we need to be at this moment is sitting with this person, with their family, to answer questions. Or sit and listen.”
The second of these most important things is “when we give of ourselves to the next generation, the same way that someone gave of themselves.” And he tied giving back into caring, as it is part of caring. Giving can take many forms. Reflecting on your teaching, updating what or how you teach. Dr. Pla recounted a story of a summer he spent at the United States Naval Academy, and a Professor of Electrical Engineering he met there. This Professor received word that a pilot had overshot the carrier deck and put their plane into the ocean. The pilot was not hurt, but this Professor asked himself “Was there something I didn’t teach that young man that had I taught him, had he known, would have prevented what could have been a fatal accident?” Hearing from graduates of the residency program about how something he taught them prevented an injury or a loss of life, particularly in airway management, reinforces that you are teaching those vital things.
When speaking with Dr. Pla it is abundantly evident that teaching is his favorite part of the work he does at GW. He lights up when talking about “The Forgotten Four,” encouraging his students to consider treatments and medications that tend to be overlooked or kept in the back of your mind, and bringing those forward. Because bringing those forward can quite literally save a life. He considers that an “ethical duty, a moral duty.” The themes of moral and ethical duties as medical practitioners echoed throughout our conversation.
Recently, Dr. Pla has made appearances on local news, encouraging the African-American community to get the COVID-19 vaccine. As one of the first people in DC to receive the vaccine, Dr. Pla says he felt an obligation to speak to his community and encourage them to get the vaccine. There is an understandable mistrust of the medical establishment within black and brown communities. Most of us can cite Tuskegee, World War II, Henrietta Lacks, Baltimore. But when we cite these infamous atrocities we overlook the personal atrocities people of color experience on a regular basis. While there is still a great deal of work to be done to rebuild that trust, to eliminate systemic racism within medicine, there is an immediate need to get vaccines to these communities that are being disproportionately affected by the virus. Because when these communities see those who have earned their mistrust saying this vaccine is the only way forward, they “[have] no hope for a better future… a pandemic-free future.” Dr. Pla sees his outreach as a way to help bring hope back to his community, to begin addressing the legacy of racism in medicine, and to hopefully earn back some trust. He hopes to continue this work in a meaningful way, to encourage colleagues and students to do their part as members of the medical community, and to address the other epidemics facing communities of color - infant mortality, maternal mortality, advanced heart disease, breast cancer, etc., all of which disproportionately affect people of color. It is “a moral calling for those of us who value lives.”
There is still so much work to be done. But, as Dr. Pla argues, just because this is a daunting task does not mean we should dismiss it. It does not mean we should despair, or give up hope. During our conversation he invoked a quote from Dr. Martin Luther King, Jr.: “The arc of the moral universe is long, but it bends towards justice.” It is a quote often invoked to remind us that the work we do today is but part of the work necessary. That the immediate is but a small part of the whole. Quite often allies, including myself at times, use this quote as an excuse to not take action when we are most needed. With Dr. Pla’s invocation, those of us who consider ourselves allies in the medical community should answer the call not to conversation, but to action. We must take steps to ensure communities of color are treated with dignity and receive a level of medical care that keeps them healthy, honoring their community-based needs and concerns.
In an effort to remain accountable to communities who have been negatively impacted by past and present medical injustices, the staff at Himmelfarb Library is committed to the work of maintaining an anti-discriminatory practice. We will uplift and highlight diverse stories throughout the year, and not shy away from difficult conversations necessary for health sciences education. To help fulfill this mission, this week’s blog post will cover Dr. Marcella Nunez-Smith.
Marcella Nunez-Smith, MD, MHS was recently appointed to chair the U.S. COVID-19 Health Equity Task Force. Dr. Nunez had been previously appointed as co-chair of the Biden-Harris transition team’s COVID-19 Advisory Board. The executive order appointing Dr. Nunez-Smith to the COVID-19 Health Equity Task Force identifies the issue that while people of color in the United States are more likely to become sick and die of COVID-19, but incomplete data on underlying health conditions, social factors, and rates of COVID-19 infection, hospitalization, and mortality have hampered an equitable response.
Dr. Nunez-Smith grew up in the U.S. Virgin Islands and pursued her education at Swarthmore College, Jefferson Medical College, and Yale University. Her understanding of the effects of limited access to health care date to her childhood when her father had a stroke in his 40s as a result of untreated hypertension. The stroke left her father partially paralyzed and Dr. Nunez Smith described the experience in a New York Times profile:
"He was a champion and a fighter. But my memories are of a father who had to live life with this daily reminder of how we had failed in terms of our health care. I don’t want another little girl out there to have her father suffer a stroke that is debilitating and life-altering in that way."
Dr. Nunez-Smith is responsible for an extensive bibliography of research on health promotion and health equity as well as research methods including primary data collection, data management and analysis, qualitative and mixed methods research, and population health. While Dr. Nunez-Smith will remain in her position as Associate Dean for Health Equity Research at Yale University and a board-certified internal medicine physician, it's her work on the COVID-19 Health Equity Task Force that is getting much attention.
Dr. Nunez Smith has identified some primary goals of the task force including addressing vaccination as well as equitable access to other healthcare services including testing, contact tracing, and treatment. In a Fortune magazine profile, Dr. Nunez-Smith discussed COVID-19 vaccination in communities of color which are historically underserved:
"It's important for us to acknowledge why there’s this hesitancy. People are going to be skeptical of vaccines, particularly many in communities where there is a not-long-ago history of experimentation, and where there are daily, contemporary reminders of differential status and access. But not every person or group that's skeptical of vaccines has their skepticism rooted in the same things, not even for every person of color who's skeptical. So we need to be thinking about targeted messaging; different people have different questions and motivations, and our response is not one-size-fits-all in terms of the information people need."
How to read a news release: Tips from the editors of JAMA
Two recent opinion pieces in JAMA address the issue of evaluating and communicating scientific information in the constantly changing era of Covid-19. Journal editors need to maintain standards of scientific integrity as they rapidly process high numbers of time-critical articles. Readers are faced with a deluge of additional information in the form of news releases, pre-prints, and blog posts – most disseminated with little review.
How should a reader approach news releases? Unlike peer reviewed articles, news releases are short and designed to grab attention. They often lack the details to conduct a traditionalcritical appraisal. Readers therefore might want to ask the following questions to make a quick assessment of the information reported in a news release:
Does the news release report on a single study?
Are main outcomes, absolute risks and patient population reported?
How does the information reported relate to other studies?
What is the context of the news release? (i.e. from a federal agency or a pharmaceutical company, designed to influence public opinion or report to stockholders)
Are the opinions of any independent experts included?
Have study results been reported elsewhere? (i.e. preprint, journals)
To learn more about critically reading a news release, check out the 10 review criteria for news stories listed atHealthNewsReview.org.
As COVID-19 cases and hospitalizations are on the rise in many US states, here are some trusted sources for tracking the situation in the DMV.
Departments of Public Health:
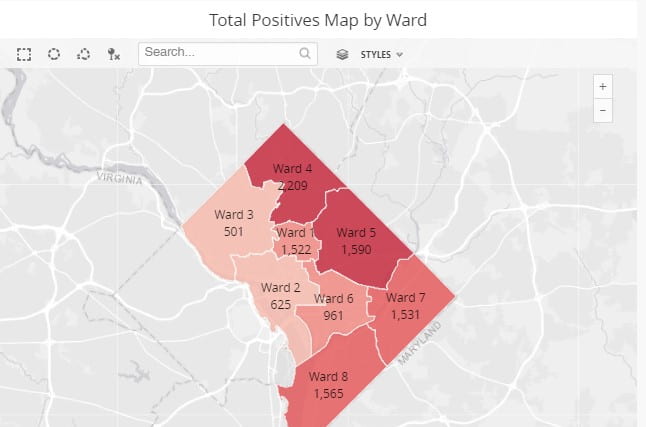
DC Coronavirus Data - Includes daily numbers tested, positives, and lives lost. Scroll down for the DC Re-Opening Tracker and data by ward, neighborhood, and demographic break outs. Tables include data for cases, quarantine and deaths of public safety personnel. Check the Press Releases area on the home page for a detailed daily summary of Coronavirus Data including trends graphs for transmission and positivity rates, and contact tracing data.
DC Hospital Status Data - Includes daily ICU, ventilator, and bed capacity, COVID hospitalization counts and total patient counts.
Maryland Coronavirus Disease 2019 Outbreak and Data Dashboard - Cases and testing by county, ICU and Acute bed capacities, percentage positive rates and testing volume 7 day averages since March 2020. Cases and deaths by age, gender, race and ethnicity.
Virginia Department of Health COVID-19 Dashboard - Includes total counts and graphic representations of cases, hospitalizations and deaths. Demographics tab provides breakouts by age, sex, race and ethnicity. Interactive localities tab provides options for counts or rates, and bar chart generation by health district and locality. Outbreaks tab shows outbreak data by setting/facility type, including long term care and correctional facilities. MIS-C tab tracks cases of Multisymptom Inflammatory Syndrome in Children by health district.
Virginia Department of Health Data Insights - Includes case and testing data by zip code, COVID-like illness visits to EDs by health regions, and modeling data from the UVA COVID-19 Model.
COVID Community Vulnerability Map - Drill down into communities by zipcode or manipulate the map to view populations most vulnerable for severe outcomes if infected with a COVID-like virus and the socioeconomic factors driving that risk.
Virginia Hospital COVID-19 Dashboard - Virginia Hospital & Healthcare Association provides counts of confirmed cases and pui currently hospitalized, ICU beds and ventilators in use, and hospitals with supply shortages.
State Health Workforce Estimator - From the Mullan Institute for Health Workforce Equity at GW, it provides state-level data for considering different strategic approaches to ensure sufficient heath workforce for COVID-19. A Contact Tracing Workforce Estimator is also available.
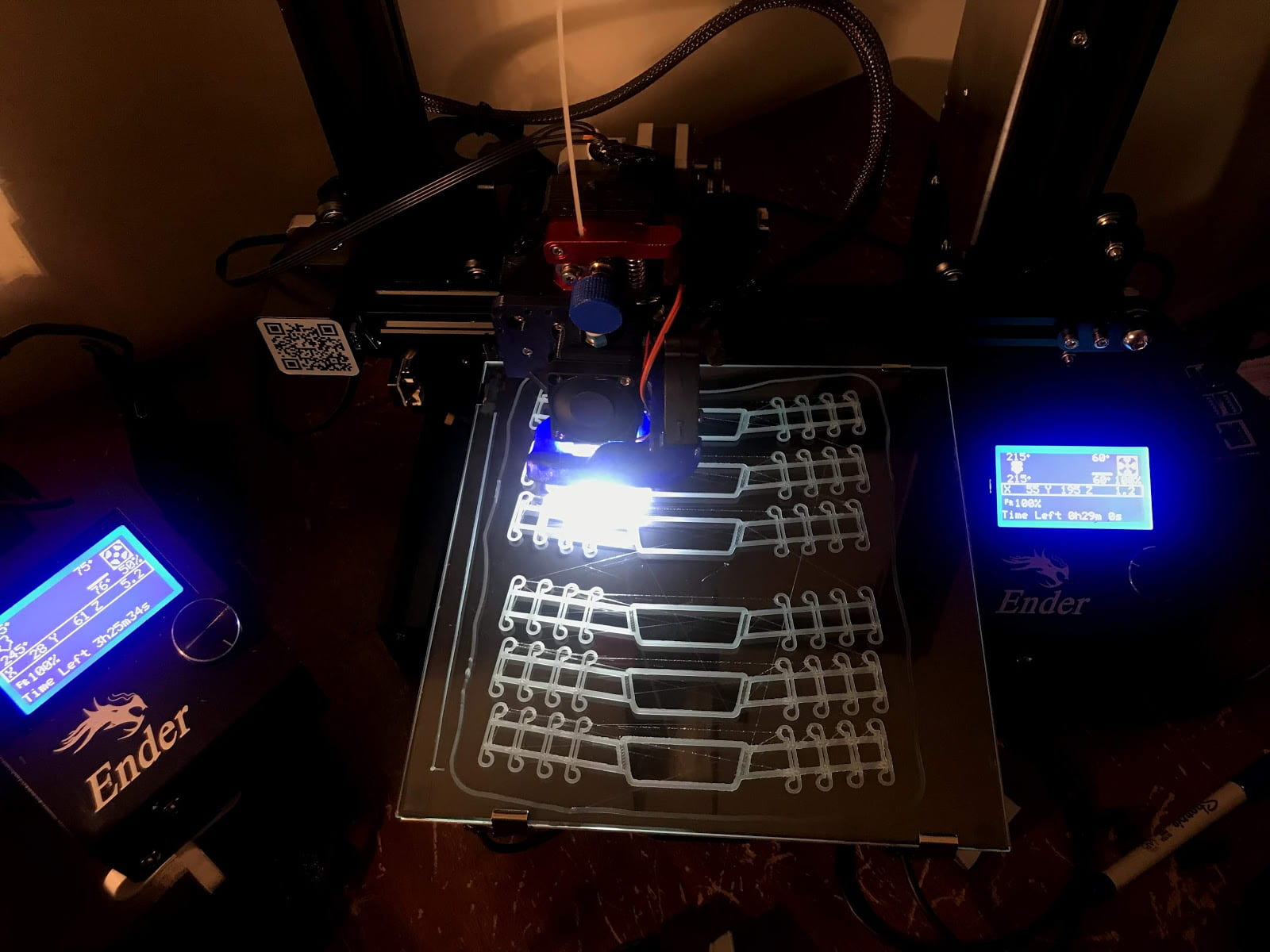
Himmelfarb Staff Member 3D Prints Face Shields for Health Care Workers
Click to watch: 3D printing process
John Lopez, Himmelfarb Library’s Data Technician, has joined an initiative to 3D print face shields for healthcare workers. John shares how he became involved in the project, and what the process entails.
How did you learn about the face shield printing initiative?
I initially read an article about a hospital in Brescia, Italy which was hit hard by the pandemic. They were running out of valves used for their respirators which the manufacturer couldn't provide quickly enough, so a small startup company reversed engineered the valve and began 3D printing them, which the hospital then used. The article quickly became viral just as COVID-19 reached the states.
I began noticing online 3D printing communities around the world organizing similar efforts once Josef Prusa - the founder of Prusa Lab in Prague, Czech Republic - released an open-source face shield design, made available for anyone with a 3D printer to produce. Various iterations were soon released, but the Prusa face shield design proved to be the most effective among health care workers.
3D-printed face shield
Are you partnering with a particular organization or initiative?
I joined the volunteer effort started by Open Works, a makerspace workshop based in Baltimore who were among the first to mobilize volunteer makers with an organized and efficient plan to provide face shields to local healthcare systems and hospitals. A chain of custody is established via email registration, as each 3D print file is assigned a unique parts number which helps keep track of how many face shields were printed by a volunteer.
What part of the shield is 3D-printed? What other materials do you need for assembly, and where can you get them? Is there a standard for what material the face shield should be made of (e.g., thickness)?
Face shield components
The face shield is actually a printable headband, as well as a printable chin strap which serves as a mount for the visor; both are included in the 3D print file. An elastic cord, along with the actual clear acrylic visor, are required to complete assembly, both of which are done at Open Works once they receive completed face shields.
PETG is the type of filament material primarily used to print the face shields, which can be purchased on Amazon for example. It's preferred due to its rigidity and because it can be sterilized more efficiently than other types of printing material such as PLA. There is indeed a printing guideline for makers to follow which sets the parameters to prevent the face shield from breaking.
How long does it take to print the shield frames?
The average print time when following the recommended print settings can take up to 6 hours for a single face shield. There are certainly a variety of ways to print faster by tinkering with hardware, such as changing the nozzle size, but it's not encouraged as strength and quality of the model are prioritized over speed.
Are you using the library’s 3D printer?
I'm grateful for my two 3D printers at home since the library's 3D printer service hasn’t been accessible.
Roughly how many have you assembled so far?
Volunteers had been asked to print at least three face shields each during the early weeks of the pandemic. The incredible response from volunteers reached a saturation point in mid-April as thousands of face shields had been made. Since then my focus has been printing ear straps for face masks.
Face shield components
Once they’re assembled, how do you get them to their destination?
Once a face shield is done printing, I wear nitrile gloves to remove the part from the print bed and follow the sanitation checklist provided by Open Works. A liability waiver is also signed then sent along with the face shields through USPS.
Is there a website (or several websites) you would recommend people visit for more information?
A good starting point for anyone with a 3D printer looking to join local volunteer efforts in their area
The expanded Research Guide is a one stop for the latest health care and public health focused news, research, literature resources, and clinical guidelines on COVID-19. It also includes the latest University news and resources for the GW health care community.
Public health and emergency management resources include tracking maps and dashboards, as well as critical resources from CDC and WHO (daily situation summaries and guidance). State and local public health department COVID-19 information and emergency management agencies are also listed.
The guide will be updated regularly and we encourage you to share any resources we’ve missed by emailing himmelfarb@gwu.edu. As always, our team of health sciences librarians is here to assist you with using any of these resources or other information needs at this time. Email us or chat usMonday-Thursday from 8:30am-8pm and Friday 8:30am-5pm.
Most of us are aware of the critical information resources on COVID-19 provided by the CDC and WHO. Many trusted publishers and literature search services in the health sciences now have devoted sites with resources for health care and public health professionals. These resources and more are now available on Himmelfarb’s Novel Coronavirus (COVID-19) Research Guide.
Here’s a sampling of resources on the guide:
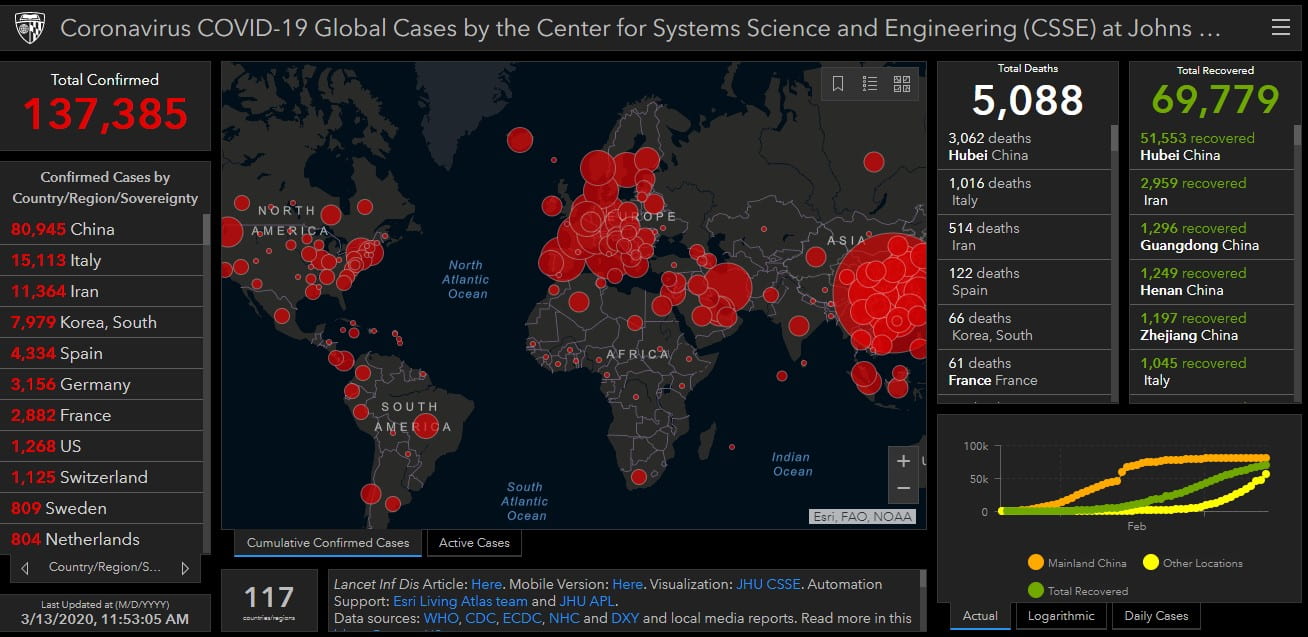
Johns Hopkins Coronavirus Dashboard - This interactive mapping service draws data from WHO, CDC, ECDC, NHC and DXY and local media reports and is constantly being updated. Track cumulative confirmed cases and active cases by country.
Novel Coronavirus (COVID-19) from DynaMed - Succinct epidemiological, diagnostic, management, and prognosis information continually updated. Includes international and US guidelines and patient information.
JAMA Network Coronavirus Disease 2019 Resource Center - Clinical information, public health preparedness, patient information, outbreak map, and multi-media CME resources. A summary of CDC guidance is at the bottom of the page.
NEJM Coronavirus (COVID-19) page - Articles, clinical reports, commentary and management guidelines published in NEJM assembled in one place. Includes a HealthMap of the outbreak.
Along with these resources you can find trusted sources for news, clinical guidelines, drug trials, health department information, and protective measures for health care professionals on the Research Guide.
Do you know of resources not included on our guide that you would like to recommend? Send them to himmelfarb@gwu.edu or jlt@gwu.edu.