GW LERNER LEARNING SERIES: FREE INSTRUCTIONAL WORKSHOPSON FITNESS FUNDAMENTALS April 1st - April 28th This series is a set of five online workshops led by fitness professionals that focuses on teaching students, faculty, and staff about health-seeking behaviors and balanced wellness in an inclusive learning environment.
CELEBRATE NATIONAL LIBRARY WEEK: READ A GOOD BOOK! April 4-10, 2021 To help you find a great book, take a look at USA TODAY’s Best-Selling Books list which ranks the 150 top-selling titles each week based on an analysis of sales from U.S. booksellers. Contributors represent a variety of outlets: bookstore chains, independent bookstores, mass merchandisers, and online retailers.
NATIONAL MUSEUM OF WOMEN IN THE ARTS IS OPEN! Open Monday thru Saturday 10AM-5PM F1250 New York Ave., NW. Admissions: Students $8.00/Adults $10. Advanced Reservations Required Located in the heart of DC, the National Museum of Women in the Arts brings recognition to the achievements of women artists of all periods and nationalities. Their collection features more than 5,500 works from the 16th century to today created by more than 1,000 artists.
In an effort to remain accountable to communities who have been negatively impacted by past and present medical injustices, the staff at Himmelfarb Library is committed to the work of maintaining an anti-discriminatory practice. We will uplift and highlight diverse stories throughout the year and not shy away from difficult conversations necessary for health sciences education. To help fulfill this mission, this week’s blog post will feature a conversation with Dr. Amanda Castel, MD, MPH.
Dr. Amanda Castel is a Professor of Epidemiology at GW. She received her BA in Biology from Brown, her MD from the University of Pennsylvania, and her MPH from Johns Hopkins. I was honored to speak with Dr. Castel about her work at GW, experiences as an infectious disease expert during a global pandemic, and her thoughts on health inequality and stigmatization.
From a young age, Dr. Castel wanted to be a doctor, and in particular a pediatrician. Born in Liberia in West Africa, Dr. Castel’s mother frequently told her about another baby born around the same time. They were both ill, but because Dr. Castel’s family is American they were able to fly her to the US for treatment. As she grew up, her family traveled internationally quite often for her parents’ work. She was able to see how other parts of the world deliver healthcare and was inspired by the idea she could “possibly make a difference and improve people’s lives.” During the course of her education, Dr. Castel took a year off to do a Fulbright Fellowship in Senegal, doing research on prevention and mother/child transmission of HIV. Through this experience, she caught the “public health bug” and decided to join her clinical interests with her public health experience. Speaking to Dr. Castel you can see her understanding of how privileged we are as Americans and her drive to create more equitable healthcare access.
After finishing her degrees, Dr. Castel worked in the CDC’s Epidemic Intelligence Service Program and was assigned to the Maryland Department of Health in their Communicable Disease Program. She describes the experience as being “a foot soldier. You are in the trenches, you’re working with county health departments… you’re doing all kinds of disease investigations.” This gave Dr. Castel the training to marry her clinical experience with her public health experience.
In early 2020, Dr. Castel watched as severely understaffed and under resourced health departments braced for the impending COVID-19 pandemic. On March 14th, 2020, Dr. Castel rolled up her sleeves, walked over to the DC Health Department, and told them “I’m here. What do you need?” In the early days of the pandemic, Dr. Castel recalls scrambling to keep ahead of the curve. The health department worked on case investigations with very limited contact tracing. The numbers were increasing so quickly they just didn’t have the bandwidth and workforce to keep up with them. As scary as those days were, from a scientific perspective they were “fascinating.” Learning how this virus worked, the transmission and symptomatology - it was a firsthand experience not many people get. Dr. Castel describes it as “professionally a very fulfilling experience.”
Alongside her work with the health department, Dr. Castel has been teaching infectious disease epidemiology at the GW School of Public Health. As part of that course, Dr. Castel tries to drive home the point that these diseases are everywhere, if you look at the news you can probably find something about an outbreak every day. January 2020, she and her students began tracking this new respiratory virus. As time went on and the pandemic progressed, these students had the opportunity to learn more about COVID within the course. When GW pivoted to online learning in March, that created a new set of challenges for educators. Dr. Castel commented on the difficulties that arise from not being in the same room as your students, that “the dynamic is different,” but even with these challenges “the students are continuing to learn and grow.” These same students are now working with health departments doing case investigations or other COVID response tasks. Those in the current cohort will be working in public health moving forward. Looking for a silver lining in times when finding them is hard, the preparation Dr. Castel gave these students is having a palpable impact on people’s lives.
Given her research in HIV/AIDS, Dr. Castel was uniquely situated to understand the ways this pandemic might unfold. In July 2020, Dr. Castel and some of her colleagues from the School of Public Health published an article discussing the synergies between HIV and COVID-19. Despite the major differences between the two viruses, it is astonishing to consider the similarities. Looking back at the beginnings of the HIV epidemic, the process of learning “which populations were most at risk, how to get testing to people, how we prevent infections, contact tracing, these core public health methods” have all been applicable to COVID-19 as well. And what we have learned through these processes are incredibly similar. The populations most disproportionately affected, racial and ethnic minorities, are the same.
Dr. Castel has researched the social ramifications of HIV, the stigmatization and public misconceptions, and the way these intersect to make treating people living with HIV harder. She does see parallels with COVID-19, especially now as vaccines become more available. Seeing the different numbers coming out from Moderna, Pfizer, and Johnson & Johnson, Dr. Castel had a genuine concern that “the general public wouldn’t understand the nuances,” and that might translate into stigmatization based on the type of vaccine being offered. It might raise questions like “If you only offer me the one that’s less effective are you discriminating against me?” And that is part of why it is so important for medical professionals and public health professionals to be able to explain these differences to the public, to understand their fears and concerns and respond to them with the facts in a way they can understand. Dr. Castel felt this especially strongly “as an African American woman working in the field,” with friends and family coming to her with their questions and concerns. Translating that information can be difficult, but it’s a vital part of the work Dr. Castel does, and a crucial part of what she teaches her students.
Despite the difficulties of the past year, Dr. Castel is hopeful. The urgency with which the scientific community responded to the pandemic has the potential to impact other areas of healthcare as well. Perhaps there will be a chance to “take some of that innovation and technology and apply it to HIV research.” But she has tempered that hope with the understanding that “the calculus is different.” COVID-19 is a pandemic that has impacted everyone, put us all at risk. The population most at risk from exposure to HIV is not one that is prioritized in the same way. It’s a stark reminder that even in the United States healthcare is not inherently equitable. Despite the fact that HIV “drastically alters the world [of those infected] in the ways that COVID has altered the rest of ours” there is an unwillingness to apply the same sense of urgency to HIV. Hopefully, as we begin to return to some sense of normalcy, those of us in the health sciences will be empowered to advocate for this kind of research. Those of us in positions of privilege who can speak to the healthcare needs of stigmatized populations need to work on communicating those needs to the general public. We can advocate for change, and call on our government to end the cycle of failing people living with HIV. We need to reevaluate our current healthcare system and public health professionals, like Dr. Castel, are ready to rise to the occasion. Of the lessons we’ve learned from the COVID-19 pandemic, one of the most important is that with a sense of urgency, adequate funding, and research, it’s possible to develop long-term solutions to viruses and diseases that still harm marginalized communities.
To learn more about the history of HIV/AIDS health policy in the US, take a look at this article covering 35 years of policy. To learn more about advocating on behalf of people living with HIV/AIDS, read this commentary from Topics in Antiviral Medicine. To learn more about Dr. Castel’s work, browse her publications indexed in the Health Sciences Research Commons.
Research is without a doubt one of the most important keys to deepening our understanding of medicine today. What we do with our research and how we publish it, is just as important as the process of research itself. It may seem like a daunting and confusing process, but it does not need to be.
At Himmelfarb Library, we have developed several resources to support you when it comes to making important decisions such selecting a journal.
Journal Selection Webinar: detailed information about how best to find a journal in your field. How to Spot a Predatory Publisher - learn the warning signs found in unsolicited emails and on journal websites that can tip you off that the journal may be predatory in nature. Preprint Servers: Balancing the Pros & Cons - preprint servers can get your research into the public sphere before publication in a journal. This video defines preprints and discusses benefits of the preprint model and some challenges that may impact scholars and researchers.
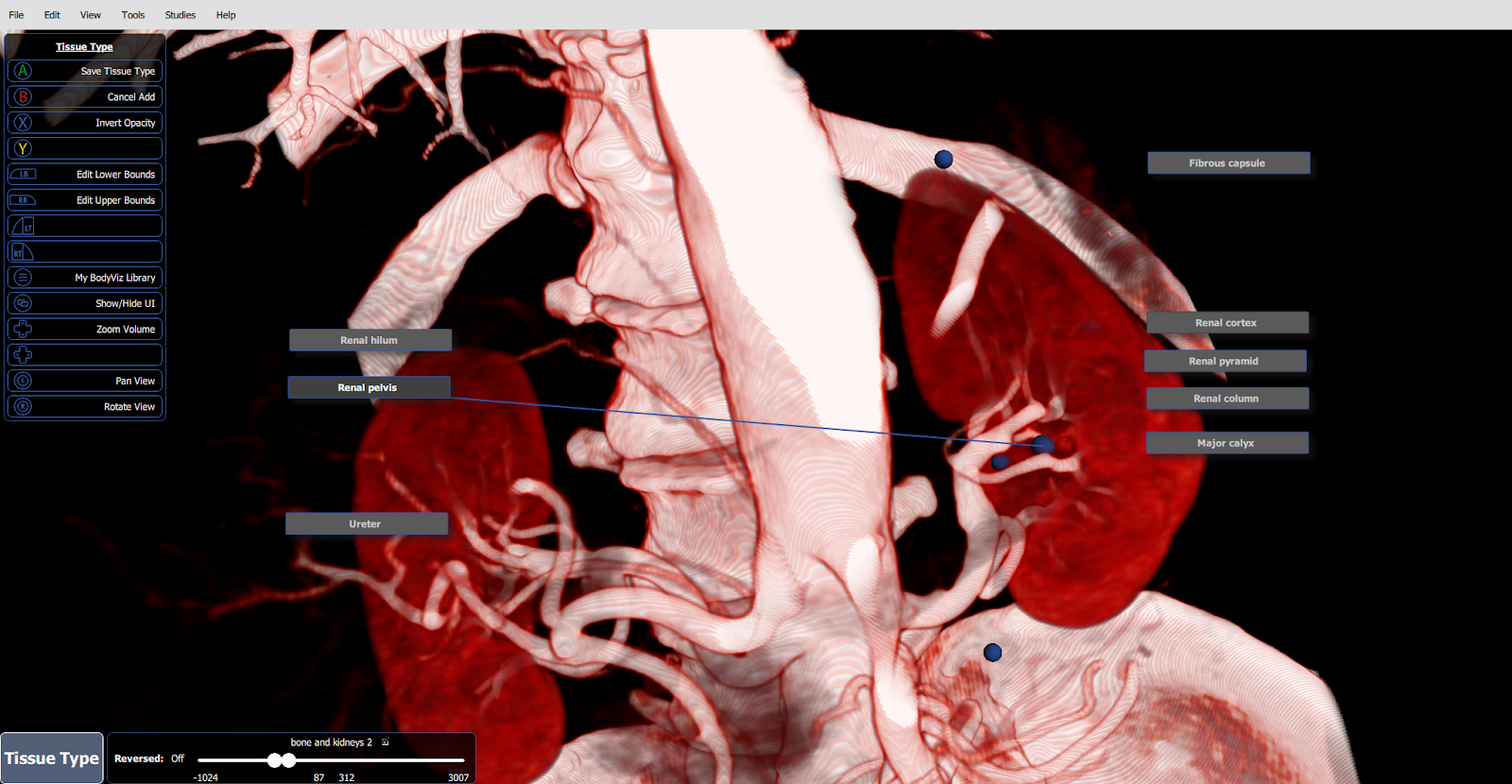
First-year medical students: we invite you to take your study of renal, GI, and liver anatomy to the third dimension!
BodyViz software, now available at Himmelfarb Library, combines digitized MRIs and CT scans to create 3D renderings of human anatomy. Enhance your learning experience during the CPR and GI/Liver blocks by exploring 360° anatomical views of kidney, gastrointestinal, and liver tissue.
Where and How?
The workstation is located at the Bloedorn Technology Center, on the third floor of the library. To use BodyViz, reserve the workstation online, and then check out the BodyViz accessories kit at the Circulation Desk on your way to the third floor.(We even include a game controller that allows you to rotate, pan, and zoom effortlessly!
Program Features
Not sure what you are looking at? Annotation mode displays labels that identify and explain anatomical structures. Want to examine deeper layers? Clipping mode allows you to peel away tissue. Want to enhance the visual display of an organ? Turn on active coloring.
Clara Bliss Hinds with the Columbian University School of Medicine Class of 1887
Clara Bliss Hinds Finley, MD was a lifelong resident of Washington,DC. Her father, Doctor Willard Bliss, served as an army surgeon in the Civil War and later ran the Armory Square Hospital.1 He is remembered for his bungled treatment of President Garfield’s gunshot wound suffered in an assassination attempt in 1881. Bliss rejected the new field of antiseptic medicine and Garfield died of septic infection after two months of repeated probing for the bullet with unsterilized hands and instruments.2
Clara was the second of Bliss’s four children and was described as an 1870’s era debutante in Washington.3 She married Jerome Hinds and they had a daughter named Bliss who would become a suffragist fundraiser and organizer.4 Clara sued for divorce after Hinds abandoned them. As a single mother in her 30s she pursued admittance to a medical school in order to support herself and her child. “A degree would mean bread and butter to me.” she told a Washington Post reporter in 1934.3
It was a hard road for 19th century women who aspired to be physicians. Few schools would admit them and it took influence and persistence to break down those barriers. Clara received support from another woman physician who helped blaze the trail before her.
“Repeated seeking for admission into D.C. medical schools brought many rebuffs, but she was given inspiration and encouragement by Dr. Mary Parsons, one of the few successful women physicians in the country at that time...”3
Dr. Parsons graduated from medical school at Howard University in 1874. When she graduated the Medical Society of the District of Columbia refused to grant her a medical license. She petitioned Congress to amend the Society’s charter to license women. The bill passed in 1875 but the Society and the AMA continued to refuse her membership for three more years. In 1878, as support for females doctors was growing, medical societies started admitting women members and granting consultation privileges.5
Clara and four other women were admitted to the Columbian University Medical School, now George Washington University School of Medicine in 1884. Of medical school, she recalled,
“They were grinding years...Competing in what was then regarded as purely man’s work, we were doing what no woman had done in the school before us. We asked no favors, and would receive none”3
Clara was the first of the women to graduate with fifty male colleagues in 1887. She and the other women who completed the program were not given opportunities for internships or residencies. Fortunately, Clara met Dr. Ida Heiberger who graduated from the Women’s Medical College of Philadelphia and did post graduate work in Europe. Together they established the Washington Women’s Clinic in 1891 at 13th and T Streets and this is where Dr. Bliss got her clinical training along with other women physicians. The clinic served indigent women and children. Clinic hours were in the evenings so working women would not have to give up a day’s wages to get care.6 The Clinic later moved to 4704 Georgia Avenue, NW and operated for 60 years.
Dr. Bliss established a successful private practice and published research on children’s growth patterns. She was a proponent of women’s physical fitness, establishing the first gymnasium for women in DC where they could remove their corsets and other constricting clothing of the day and move freely. Serving as the gym’s medical director helped to supplement her income.7
Clara married again in 1894 to Henry Jennings Finley, a Washington, DC attorney. That year she and a group of other prominent women founded the Business Women’s Club of Washington DC.4 Her involvement in professional societies and how they aided her education and career is the focus of a paper currently being researched by a group at SMHS including Dr. Kirsten Brown, Professor of Anatomy, Dr. Victoria Shanmugam, Director of the George Washington University Division of Rheumatology, Dr. Nadine Mbuyi, Assistant Professor of Medicine, and Sara Hoover, Himmelfarb Library’s Scholarly Communications and Metadata Librarian.
Dr. Bliss died in 1940 and is buried in Rockville Cemetery alongside Henry and her daughter Bliss.8
Today Dr. Bliss is honored as the namesake of the Clara Bliss Hinds Society for Women in Medicine and Science at GW. The group oversees programs that help to support women faculty including regular meetings and an Annual Women in Leadership Event. On April 14th the Society will host a program on Achieving Gender Equity in Compensation and Career Advancement via Webex from 5-6pm.
4. Hammond W and LaBrie A. Biographical Sketch of Bliss Finley, 1881-1970. Biographical Database of Militant Woman Suffragists, 1913-1920. Alexandria, VA: Alexander Street Press, 2015. https://documents.alexanderstreet.com/d/1008297916
6. Hildebrand JR. Woman’s Clinic Has Blazed Path for Medical School for Women Physicians. The Washington Times Home Edition, August 19,1914. https://chroniclingamerica.loc.gov/lccn/sn84026749/1914-08-19/ed-2/seq-8/
7. Creese, MRS. Clara Bliss Hinds. Ladies in the Laboratory? American and British Women in Science, 1800-1900: A Survey of their Contributions to Research. Lanham, MD: Scarecrow Press, 1998. p. 166
In case you haven’t noticed, Spring is just around the corner! After a long winter filled with hearty and savory recipes, it is time to enjoy what the flourishing season has to offer!
Are you looking to zest up a chicken dish? This Crispy braised chicken thigh recipe includes artichokes, tarragon and leeks, all of which are in season! Never cooked with an artichoke before? Don’t worry, there are highly detailed photos and instructions that show you how to turn the leafy green globe into goodness!
For all of you vegetarians out there, EatingWell has a White Bean & Avocado salad that requires absolutely no ranch dressing! Additionally, this vegan BBQ Pizza with crispy cauliflower combines a bold flavor with unique toppings that will surely satisfy any who are looking to try something new.
If you are trying to avoid sugar but are craving something sweet, Simplysohealthy has a Sugar Free Strawberry Lemonade that only requires four ingredients to make! In similar fashion, this Blueberry-Lemon Ricotta pound cake can be made in a single bowl. Talk about a perfect treat to brighten any spring afternoon.
We wish you a warm, safe and healthy spring season filled with many colorful and new dishes!
New Publication from GW Researchers Highlights Link Between Aspirin use and Decreased COVID-19 Severity in Hospitalized Patients
A recent clinical research report led by Jonathan H. Chow, Assistant Professor of Anesthesiology and Critical Care Medicine at the George Washington University, found that the use of aspirin may be associated with improved outcomes for hospitalized COVID-19 patients. The study entitled Aspirin Use Is Associated With Decreased Mechanical Ventilation, Intensive Care Unit Admission, and In-Hospital Mortality in Hospitalized Patients With Coronavirus Disease 2019 was published in the journal Anesthesia & Analgesia tracked 412 adult patients with COVID-19 and suggests that aspirin may provide lung-protective effects that help reduce the need for mechanical ventilation and ICU admissions. The article was featured in a recent news release from the American Association for the Advancement of Science. A randomized control trial is now needed to assess whether there is a causal relationship between aspirin use and a reduction in lung injury among COVID-19 patents.
Have you wondered what an article’s citation count means? Who cited the article? How?
Take the now-retracted Wakefield et al. article “Ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children” (1998). Though most citations are negative, this is not reflected in the overall citation count (Suelzer, 2019). A unidimensional metric like citation count does not capture the diversity of how and where citations appear.
Scite aims to contextualize the citation count
Scite, founded by Josh Nicholson and Yuri Lazebnik and previously funded by NSF and NIDA, is a database of over 800 million citation statements (Herther, 2021) categorized as
Supporting: providing supporting evidence for the cited work
Mentioning: mentioning the cited work
Disputing: providing disputing evidence for the cited work
The statements are also tagged by where they appear in citing articles (intro, results, methods, discussion, or other).
Scite uses text mining and artificial intelligence
Scite uses machine learning to enhance the database of citation statements. “The corpus on which the model was trained included 43,665 citation statements classified by trained annotators with experience in a variety of scientific fields” (Nicholson et al., 2020). Scite continues to build partnerships with publishers to gain access to articles for text mining. While the tool is imperfect and evolving, it begins to demonstrate how and where works are being used.
Publishers and researchers can use scite
In addition to citation counts and altmetrics, scite smart citations are beginning to appear on databases and journal websites. They are already available in EuropePMC records (Herther 2021, Araujo & Europe PMC, 2020).
Researchers also use scite to see how others use their own publications and how their results fit into the larger landscape. With a free account, researchers can create a limited number of reports and visualizations and set up author alerts. Researchers can use the digital badge when presenting their works. A paid account provides access to the reference check feature, which alerts authors to potentially disputed or retracted references in an uploaded manuscript.
Finally, the founders of scite hope that smart citations will encourage researchers to “report unsuccessful attempts to [test] reported claims, as so called negative results often go unpublished because they are considered inconsequential” (Grabitz et al., 2017).
Use scite with a grain of salt
The technology is evolving and the corpus to which scite has access is incomplete. As with all citation indexes, the methods and data sources vary, which is why different numbers are found across platforms like Scopus, Web of Science, PubMed, and Google Scholar. Scite’s founders caution users “given the limitations of the model precision [and] the current limited coverage of articles analyzed by scite” (Nicholson et al., 2020).
Take the Wakefield et al. (1998) article. As of March 8, 2021, the article has been cited by 349 articles in PubMed, 1,443 in Web of Science, 1,590 in Scopus, and over 3,000 in Google Scholar. The scite browser plug-in shows over 1,000 citation statements (note one citing article may include multiple citation statements). Most are classified as mentions, with 2 confirming and 7 disputing (See: A retracted article has no disputing cites, does that mean scite is not working? | scite help desk). In contrast, a recent analysis found 838 negative citations in a collection of 1,153 citing works (Suelzer et al. 2019).
Methods and tools to evaluate research and improve reproducibility continue to evolve, and researchers can contribute to improving the model by flagging mis-classified citations. While many AI-based tools are still in development, they offer hope for a multidimensional approach to publication metrics.
Grabitz, P., Lazebnik, Y., Nicholson, J., & Rife, S. (2017). Science with no fiction: Measuring the veracity of scientific reports by citation analysis [Preprint]. Scientific Communication and Education. https://doi.org/10.1101/172940
Nicholson, J. M., Uppala, A., Sieber, M., Grabitz, P., Mordaunt, M., & Rife, S. C. (2020). Measuring the quality of scientific references in Wikipedia: An analysis of more than 115M citations to over 800 000 scientific articles. The FEBS Journal, febs.15608. https://doi.org/10.1111/febs.15608
Suelzer, E. M., Deal, J., Hanus, K. L., Ruggeri, B., Sieracki, R., & Witkowski, E. (2019). Assessment of citations of the retracted article by wakefield et al with fraudulent claims of an association between vaccination and autism. JAMA Network Open, 2(11), e1915552. https://doi.org/10.1001/jamanetworkopen.2019.15552
Wakefield, A., Murch, S., Anthony, A., Linnell, J., Casson, D., Malik, M., Berelowitz, M., Dhillon, A., Thomson, M., Harvey, P., Valentine, A., Davies, S., & Walker-Smith, J. (1998). RETRACTED: Ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children. The Lancet, 351(9103), 637–641. https://doi.org/10.1016/S0140-6736(97)11096-0
In an effort to remain accountable to communities who have been negatively impacted by past and present medical injustices, the staff at Himmelfarb Library is committed to the work of maintaining an anti-discriminatory practice. We will uplift and highlight diverse stories throughout the year, and not shy away from difficult conversations necessary for health sciences education. To help fulfill this mission, today's blog post will cover Clara Barton.
Clara (Clarissa) Harlowe Barton, is perhaps best known as the founder of the American Red Cross. But Barton’s impact stretches far beyond her work with the Red Cross. “Her intense devotion to serving others resulted in enough achievements to fill several ordinary lifetimes” (American Red Cross, n.d.).
Born in 1821 in North Oxford, Massachusetts, she was the youngest of five children. When she was 11 years old, an older brother was seriously injured in a fall. Barton spent two years nursing him back to health until he was fully recovered. While Barton would never have any formal training as a nurse, this experience proved to be indispensable. She later wrote about the experience stating:
“I learned to take all directions for his medicine from his physician…and to administer them like a genuine nurse. My little hands became schooled to the handling of the great, loathsome, crawling leeches which were at first so many snakes to me, and no fingers could so painlessly dress the angry blisters; and thus it came about, that I was the accepted and acknowledged nurse of a man almost too ill to recover.”
Despite this early nursing experience, Barton would not embrace a nursing career until later in life. At the age of seventeen, Barton worked as a teacher in North Oxford, Massachusetts (Clara Barton Birthplace Museum, 2017). Twelve years later, she opened the first free public school in Bordertown, New Jersey (Clara Barton Birthplace Museum, 2017). The school grew from only six students on the first day of classes to more than 200 students by the end of the school year (Clara Barton Birthplace Museum, 2017). When the school opened in the fall of 1853, Barton was shocked to learn that a man had been hired as the school’s principal, earning twice her salary to run the school that she had founded and made successful. Outraged at this news, she resigned her teaching position. “I may sometimes be willing to teach for nothing, but if paid at all, I shall never do a man’s work for less than a man’s pay” she proclaimed.
The following year, Barton moved to Washington, D.C. to be “one of only a few female clerks at the US Patent Office and the only woman in her office receiving a salary equal to the male clerks” (National Park Service, 2020). As one of the first women employees of the federal government, she faced harassment from her male colleagues who “tried to besmirch her good name and get her fired” (National Park Service, 2020).
In 1861, Barton moved into a boarding house on 7th St., now the site of the Clara Barton Missing Soldiers Office Museum. The Civil War had just begun, and Barton saw a need for providing supplies and personal assistance to men in uniform. She began collecting supplies and obtained passes from the government to deliver her supplies and services to the front lines and field hospitals. After appearing “at a field hospital at midnight with a wagon-load of supplies,” she became known as the “Angel of the Battlefield” (American Red Cross, n.d.). She nursed, comforted, and cooked for the wounded often at great personal risk to her own safety. On one account, “as she knelt down to give one man a drink, she felt her sleeve quiver. She looked down, noticed a bullet hole in her sleeve, and then discovered that the bullet had killed the man she had been helping” (National Park Service, 2020).
As the war drew to a close, Barton often found herself responding to letters from family members looking for missing soldiers. Again seeing a need, Barton established the Office of Correspondence with Friends of the Missing Men of the United States Army. Barton and her assistants received and answered more than 63,000 letters and identified more than 22,000 missing men. Some of these men were still alive. Years later, the “Red Cross established a tracing service, one of the organization’s most valued activities today” (American Red Cross, n.d.).
In 1869, Barton took a trip to Switzerland where she learned about the International Red Cross. Barton appealed to three sitting US Presidents to sign the Geneva Treaty (American Red Cross, n.d.). In 1882, President Chester Authur signed the treaty, and it was ratified by the Senate (American Red Cross, n.d.). Under Barton’s leadership, the American Red Cross helped victims of forest fires in Michigan, survivors of the Johnstown flood, famine in Russia, hurricane and tidal wave relief in a predominantly African-American community in the Sea Islands of South Carolina just to name a few (American Red Cross, n.d.). “The American Red Cross, with Barton at its head, was largely devoted to disaster relief for the first 20 years of its existence” (American Red Cross, n.d.).
A Red Cross supply warehouse in Glen Echo, Maryland served as the first permanent headquarters of the Red Cross, as well as Barton’s home. She lived here for the last 15 years of her life until her death on April 12, 1912. This site is now the Clara Barton National Historic Site. While this site is currently closed due to the pandemic, it is well worth touring if you have the opportunity in the future.
In 1904, at the age of 82, Barton stepped down from the Red Cross. Today’s American Red Cross still focuses on providing disaster relief, and the mission has been expanded to include: providing lifesaving blood through their blood donation program; providing training and certification courses in lifesaving skills such as first aid, CPR, and AED use; providing international disaster relief services; and helping military families prepare for and cope with the challenges of military service.
During her lifetime, Barton was also a strong supporter of women’s rights. She supported suffragists such as Susan B. Anthony, Elizabeth Cady Stanton, and Frances D. Gage, and often spoke publicly in favor of equal rights for women (Clara Barton Missing Soldiers Office Museum, 2021). Barton dedicated her life to the service of others as a teacher, a Civil War nurse, and founder of the American Red Cross. By dedicating her life to the care of others, she left a legacy of caregiving and disaster relief in America and abroad.
Highsmith, C.M., photographer. Clara Barton’s Home, Glen Echo, Maryland. United States Maryland Glen Echo, None. [Between 1980 and 2006] [Photograph] Retrieved from the Library of Congress, https://www.loc.gov/item/2011631520/





 (All images courtesy: of Aalap Herur-Raman, MSI)
(All images courtesy: of Aalap Herur-Raman, MSI)