August is National Immunization Awareness Month (NIAM). Regular immunizations are an important part of staying healthy. Vaccines help provide immunity before potential exposure to diseases. Vaccines help your body create antibodies to fight off infections by training your immune system to recognize and destroy harmful pathogens before they can cause serious illness. To learn more about how vaccines work, check out this great video from Nature - which you can also share with your patients:
Himmelfarb Library also has a number of immunization resources available! Next time you’re in the library, check out our current book display on the first floor with immunization and vaccine-related resources. If you see something of interest, ask at the circulation desk to check out the book.
We also have some great e-books available on the topic of vaccines:
Plotkin’s Vaccines: by Walter A. Orenstien et. al. is an award-winning 2024 text that provides the latest vaccination evidence, recommendations, and protocols.
The Ethics of Vaccination: by Alberto Guibilini discusses individual, collective, and institutional responsibilities surrounding vaccination from a philosophy and public health ethics point of view.
Gun violence is a public health crisis in the United States. According to a July 2023 report from the Kaiser Family Foundation, which was based on data from the Centers for Disease Control and Prevention (CDC) WONDER database, firearms were involved in more child deaths in 2020 and 2021 than any other cause (Matt McGough, Krutika Amin, & Nirmita Panchal, 2023). The United States has the highest rate of firearm mortality among children and teens compared to peer countries (U.S. has the highest rate of gun deaths for children and teens among peer countries, 2023).
The CDC data is useful, but there is a time lag associated with the availability of this data. For those looking to track the effects of gun violence in close to real-time, there is the nonprofit Gun Violence Archive (GVA). Media outlets, which rely on up-to-the-minute sources of data, have grown to depend on the detailed information about gun violence that is being continually compiled and updated by GVA for news reporting purposes.
While “gun violence” was established as a MeSH term only in 2019, GVA was established in 2013, by Mark Bryant and Michael Klein (Drenon, 2023). The GVA’s database contains gun violence incident reports collected from “over 7,500 law enforcement, media, government, and commercial sources daily in an effort to provide near-real-time data about the results of gun violence” (GVA, n.d.). GVA is unique, in that it is an independent data collection and research group with no affiliation with any advocacy organization.
Bryant, who runs the GVA from his home in Kentucky, might seem an unlikely founder of a research database on gun violence. As he told a BBC interviewer earlier this year, he began shooting at age five, and he has amassed a collection of guns passed along by family members. "Somebody has made the assumption that I'm doing this project that I must be against guns but lo and behold, I own guns," Bryant told the BBC, clarifying that his personal collection includes handguns, pistols, and revolvers – but no assault weapons. GVA initially began as a collaboration with Slate Magazine, because founder Bryant kept finding and reporting missing data in the daily tally of gun violence statistics that Slate began keeping following Sandy Hook (Matt Drange, 2016). GVA eventually emerged as an independent website with financial support from Michael Klein, founder of the now-defunct Sunlight Foundation, which strove to use civic technology, open data, policy analysis, and journalism in order to increase transparency and accountability in government and politics.
The GVA website is updated continuously, and an interactive map is associated with the incidents, the sources of which are included (typically local media reports). This searchable map includes statistics by date ranges on shootings including mass, accidental, officer-involved, child-involved, and fatal and non-fatal shootings from 2014-2022.
Data from the Gun Violence Archive underlies this interactive atlas of gun violence incidents in the United States, beginning with 2014 and current through the end of 2022. (Image source: The Trace, Gun Violence Archive)
Reports from GVA are available on a variety of topics, and can be exported as CSV documents or displayed as maps
National Healthy Vision Month is an annual reminder of the importance of prioritizing our eye health and well-being. Throughout July, individuals and organizations come together to raise awareness about the significance of a healthy lifestyle, preventive care, and the pursuit of wellness for all. Let's explore the essence of Healthy Vision Month and discover how to help protect your vision.
Healthy Vision Month serves as a platform to educate, motivate, and inspire people to make informed choices regarding their vision health. It emphasizes the significance of preventive measures, regular check-ups, and self-care practices that contribute to long-term well-being. By spreading awareness, we empower individuals to take control of their health and work towards healthier futures.
If you are uncertain of how to begin, make sure you are taking some simple steps to keep your eyes healthy. This includes encouraging physical activity, proper nutrition, stress management, and adequate sleep. Small changes in daily habits can have a significant impact on overall health. By incorporating healthy practices into our routines, we enhance our quality of life and reduce the risk of preventable diseases.
For further information, you can check out some of Himmelfarb’s resources:
It has been over a year since the Supreme Court issued its decision in the case Dobbs v. Jackson Women’s Health Organization. The Dobbs decision overturned the 1973 Roe v. Wade opinion and determined that the U.S. Constitution does not confer a right to abortion and returned the authority to regulate abortion to individual states. Currently, 15 states have laws that prevent access to abortion and 11 other states impose a gestational limit on abortion care. (Abortion Policy Tracker, 2023) Due to the patchwork of state laws and local ordinances that cover abortions, individuals with reproductive healthcare needs may encounter difficulties when searching for the best care or they may face barriers in accessing information about abortion. These barriers impact an individual’s overall health and can feed into our larger understanding and acceptance of abortion, reproductive health and reproductive justice.
Researchers created the term ‘abortion stigma’ to explain how the silence and wariness around discussing abortion impacts individuals, healthcare providers, activists and others. Barbara Alvarez writes “When people can’t access credible health information, they can’t make the best decisions for their mental and physical wellbeing. That’s why the World Health Organization (WHO) includes information access as one of its three cornerstones for comprehensive abortion care.” (Alvarez, 2022, para. 1) Dismantling ‘abortion stigma’ is not only a healthcare concern, but also an information access concern that healthcare and information professionals should address.
Kumar, Hessini & Mitchell define abortion stigma “as a negative attribute ascribed to women who seek to terminate pregnancy that makes them, internally or externally, as inferior to ideals of womanhood.” (Kumar, Hessini & Mitchell, 2009, pg. 628) The authors also note that abortion stigma “is a social phenomenon that is constructed and reproduced locally through various pathways.” (Kumar, Hessini & Mitchell, 2009, pg. 628) Norris et al. expands this definition so that it includes others who are impacted by this form of stigma. “Secrecy and disclosure of abortion often pertain to women who have had abortions, but may also apply to other groups–including abortion providers, partners of women who have had abortions, and others–who must also manage information about their relationship to abortion.” (Norris et al., 2011, pg. S50)
There are layers to abortion stigma and how it appears in people’s lives. For example, Norris et al. note that “Legal restrictions (e.g., parental consent requirements, gestational limits, waiting periods, and mandated ultrasound viewing) in the United States make it more difficult for women to obtain abortions and reinforce the notion that abortion is morally wrong.” (Norris et al., 2011, pg. S51) Abortion stigma may prevent healthcare professionals from pursuing coursework or a career in abortion care or this stigma may have a negative impact on the health of the provider. “Physicians who are trained to but do not provide abortions describe explicit and subtle practice restrictions and fear of repercussions from colleagues.” (Norris et al., 2011, pg. S51) Information specialists, such as librarians and other library professionals, may also hesitate to include information about abortion in their institutions’ collection because the inclusion of these resources may be challenged. Or, they may be unaware of the need for abortion resources as abortion stigma and library anxiety compounds and prevents patrons from seeking assistance from librarians or other staff members. “I received feedback from librarians that described the post-Dobbs landscape: they replied that patrons may have “fear and uncertainty of how to protect [themselves] if [they] are seeking abortions services.”” (Alvarez, 2023, para. 3)
Without reliable access to accurate information, people cannot make informed decisions about their health. This information is also important because it challenges the negative connotations associated with abortion or other stigmatized procedures. Norris et al. proposed that normalizing abortion as a solution to dismantling this stigma: “We should engage popular media, including popular entertainment, in the effort to remind people that abortion is common and usual.” (Norris et al., 2011, pg. S53) One way of doing this is by eliminating restrictions in information access and affirming the basic right to information and intellectual freedom. “...although there are many ways to approach intellectual freedom in libraries, there is often a common theme of human dignity that appears either explicitly or between-the-lines…all of these perspectives rely on the autonomy of each patron and their ability to exercise that autonomy.” (Childs, 2017, pg. 65)
If you wish to participate in the dismantling of abortion stigma, organizations such as the Guttmacher Institute, SisterSong Women of Color Reproductive Justice Collective, KFF provide resources on abortion, current legislation and other key pieces of information. These organizations will equip you with information to navigate conversations on abortion and reproductive justice.
Additionally, if you are interested in learning more about intellectual freedom and would like to assist library professionals with building inclusive collections, the American Library Association (ALA) has dedicated resources available. Their Intellectual Freedom: Issues and Resources page is an excellent starting point. Or, you can learn how to support library workers as they work to ensure intellectual freedom within their institutions by visiting the ALA’s Fight Censorship page.
Finally, Himmelfarb Library has materials on reproductive health and reproductive justice. For assistance answering specific questions or finding resources, use our Ask a Librarian service to speak with a reference specialist who can connect you with resources.
Dismantling abortion stigma requires a collaboration between healthcare and information professionals. If people are required to make decisions about their reproductive health, they must have access to information without undue restrictions. By working together to address this stigma, healthcare and information professionals can empower people to make informed decisions.
Childs, L. (2017). To Uphold and Resist: Protecting Intellectual Freedom through Progressive Librarianship. The Serials Librarian, 73(1), 58–67. https://doi.org/10.1080/0361526X.2016.1270248
Kumar, A., Hessini, L., & Mitchell, E. M. H. (2009). Conceptualising abortion stigma. Culture, Health & Sexuality, 11(6), 625–639. https://doi.org/10.1080/13691050902842741
Norris, A., Bessett, D., Steinberg, J. R., Kavanaugh, M. L., De Zordo, S., & Becker, D. (2011). Abortion Stigma: A Reconceptualization of Constituents, Causes, and Consequences. Women’s Health Issues, 21(3), S49–S54. https://doi.org/10.1016/j.whi.2011.02.010
Image by Gerd Altmann from Pixabay https://pixabay.com/illustrations/digitization-healthcare-health-6939536/
Artificial intelligence is on the cusp of radically transforming many aspects of our lives, including healthcare. AI tools can be used to aid diagnosis, recommend treatments, and monitor patients through wearables and sensors. A study published in May of this year found 47 FDA-approved AI remote patient monitoring devices. The majority monitor cardiovascular functions, but the study also found diabetes management and sleep monitors (Dubey and Tiwari, 2023).AI-enabled surgical robots are in various phases of testing and adoption. Partially autonomous systems like da Vinci and TSolution One® are in use for hard tissue procedures and the NIH reported on the successful use of a soft tissue robot last year (Saedi, et al., 2022).
AI can track trends in health or make predictions about it in populations. For example, the earliest warnings about the Covid pandemic came from two AI applications, HealthMap and BlueDot in December of 2019 (Chakravorti, 2022). A recent editorial in Pathogens discusses how AI machine learning can be used to analyze large data sets to identify patterns and trends in infectious disease, identify potential drug targets, and build predictive models to prevent or mitigate outbreaks (Bothra, et al., 2023).
AI administrative tools can greatly reduce the burden of paperwork through digital note taking with speech recognition software and filing insurance claims with systems like Medicodio. They can also be used to optimize scheduling, staffing, and resource allocation. AI robots that can gather and deliver supplies and equipment, reducing the burden on nurses and other clinical staff, are being adopted in hospitals (Gaines, 2023).
A 2020 GAO report on AI in healthcare identified challenges to building effective and safe AI applications. Accessing quality data headed the list. Incomplete and inconsistent data sets hampered AI decision tools during the Covid pandemic response (Chakravorti, 2022). Bias in data, lack of transparency, risks to patient privacy, and potential liability were also identified as barriers.
Another important factor is lack of trust in or acceptance of AI applications in healthcare by health consumers. A recent Pew Survey found that 60% of Americans are uncomfortable with AI being used in their healthcare and fewer than half believed that AI would improve health outcomes. The findings were not all negative. A majority thought that AI would reduce the number of mistakes made by healthcare providers and that it could also help eliminate bias and unfair treatment in healthcare. Respondents were comfortable with AI tools for skin cancer detection, but decidedly less comfortable with AI surgical robots and use of chatbots for mental health screenings. They were also concerned that the pace of adoption of these technologies will be too fast before risks to patients are understood and minimized.
References
Dubey, A. and Tiwari, A. (2023). Artificial intelligence and remote patient monitoring in US healthcare market: a literature review. Journal of Market Access & Health Policy, 11(1), 2205618. https://doi.org/10.1080/20016689.2023.2205618
Saeidi, H, Opfermann, J.D., Kam, M, et al.(2022). Autonomous robotic laparoscopic surgery for intestinal anastomosis. Science Robotics 7(62). https://doi.org/10.1126/scirobotics.abj2908
Bothra, A., Cao, Y., Černý, J., & Arora, G. (2023). The Epidemiology of infectious diseases meets AI: a match made in heaven. Pathogens, 12(2), 317. https://doi.org/10.3390/pathogens12020317
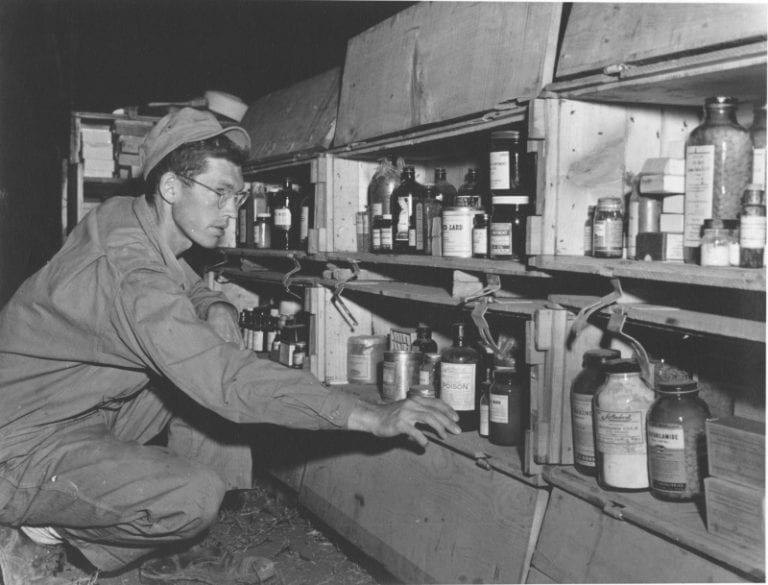
Health care personnel have assisted military units for centuries, both in unofficial capacities and as recognized members of the armed forces. Whether they were actively treating injured soldiers on the frontline or performing complex surgeries in military hospitals, physicians, surgeons, nurses and other health professionals worked alongside soldiers and commanders to ensure that the injured were properly treated.
Prior to the 19th and 20th centuries, healthcare treatment within the military was largely decentralized and relied on inaccurate information on wound treatment and patient care management. But as more advanced weapons and military tactics were introduced, countries and military leaders invested in their healthcare infrastructure which led to lower mortality rates and the decrease of widespread infection within military camps. Many of the inventions introduced during conflicts such as the Napoleonic Wars, the American Civil War and the World Wars have been carefully refined and serve as the foundation for today’s current military medicine practices.
Health and medicine have been the focus of research for centuries. Many ancient historical figures and civilizations documented their theories about human anatomy, physiology, the nature of diseases and health remedies. Preserved historical texts from ancient civilizations provide us with a glimpse of some of the health treatments and theories proposed by scholars. In Homer’s The Iliad, surgeons were portrayed as “skilled and professional physicians who expertly treated wartime trauma.” (Manring et al., 2009, pg. 2173) Ancient Egyptians and Babylonian-Assyrians left behind texts and treatises that showed cultures with sophisticated and thoughtful ideas about medicine and the human body. (Van Way, 2016)
During the time of the Roman Empire, “The Roman army had organized field sanitation, well-designed camps, and separate companies of what we would now call field engineers. They had a much better grasp of sanitation and supply than anyone else before, or for a long while.” (Van Way, 2016, pg. 260) While ancient civilizations lacked the technology and scientific theories that form the foundation of modern medicine, these cultures worked to protect their injured soldiers during battle. Some civilizations, such as the Romans, understood the importance of maintaining clean environments to prevent epidemics from debilitating their armed forces. As Dr. Charles Van Way III wrote, “Because of their [The Romans] improved sanitation, their armies suffered somewhat less from the epidemics which swept military camps, but only by comparison with their opponents.” (Van Way, 2016, pg. 261)
Unfortunately, when the Roman Empire fell, their ideas on sanitation and healthcare management were lost. For years, there were few scientific advances and many physicians relied on the ancient and incorrect humoral theory or four humors theory which was first suggested by the Ancient Greeks. According to this theory, the human body consisted of four ‘humors’: black bile, yellow bile, blood and phlegm. If a person was ill, humoral theorists believed the sickness was caused by an imbalance of humors within the body, instead of pathogens or forces outside the body. While there are some critics of this theory, it was the prevailing medical belief until the 18th and 19th centuries.
With the development of the scientific method around the 17th century, empirical observations became the basis for theories; the humoral theory eventually fell out of favor and more evidence-based practices/theories took its place. This impacted military medicine as healthcare responders developed new techniques that contributed to declining mortality rates and a more sanitary wound treatment management system.
Some discoveries and resources that were developed during this time include Jean Louis Petit’s tourniquet, Pierre-Joseph Desault’s description of the debridement of wounds and the publication of three textbooks on military medicine. (Van Way, 2016, pg. 262) But it was during the Napoleonic Wars (1792-1815) where military medicine began to improve and leaders recognized the importance of a well maintained military healthcare system. Baron Dominique-Jean Larrey is seen as the originator of modern military medicine. Some of his contributions to the field include an early framework for the triage system, the “ambulance volante” or flying ambulance and the use of field hospitals that were located away from the battlefield. (Van Way, 2016; Manring et al., 2009)
Despite the recommendations created by Baron Dominique-Jean Larrey, armies still failed to create an organized healthcare system within their military. This caused controversy during some campaigns. For example, during the American Civil War (1861-1865) both the Union and Confederate armies “had physicians, but there was only a rudimentary hospital and evacuation system…Public health was terrible. Many soldiers died of disease, often even before reaching the battlefield.” (Van Way, 2016, pg. 336) This eventually led to the establishment of a military medical corps that treated the injured soldiers. And during the Crimean War (1853-1856), public outrage over the treatment of wounded British soldiers led the War Office to enlist the services of Florence Nightingale. Nightingale and her staff of volunteers focused on sanitation, ventilation and waste disposal. Because of her efforts, she “broke the monopoly of health care as the sole providence of the physician, which led to the development of the healthcare team in modern medical practice.” (Manring et al., 2009, pg. 2169)
Military medicine faced its greatest challenge during the world wars and the field continued to shape itself into the modern version that is present today. When the U.S. joined World War I (1914-1918), hospitals, doctors, nurses and ambulances accompanied the soldiers and commanders. Ambulances were used to transport the wounded from the battlefield, and from there the soldiers would be taken to a healthcare team or moved to a facility where they could recover. (Van Way, 2016) Between the wars, medical advancements were incorporated in the field of military medicine such as “Blood and plasma transfusions, widespread use of intravenous fluids, antibiotics (but limited to penicillin and sulfonamides), endotracheal intubation, thoracic and vascular surgery, and the care of burn wounds.” (Van Way, 2016, pg. 338)
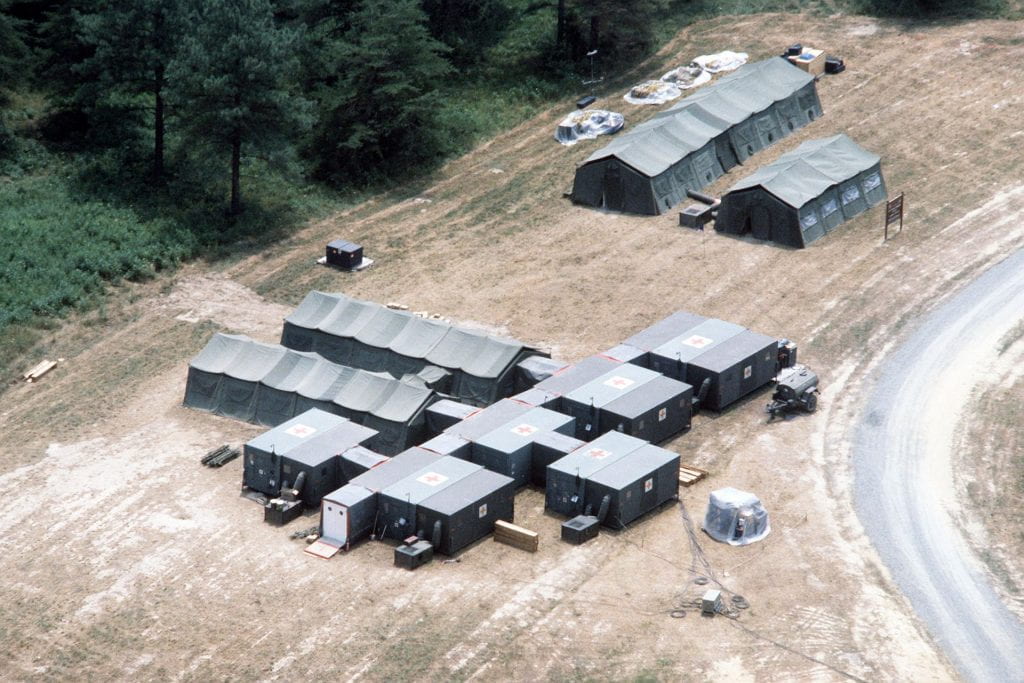
Military medicine was further tested during conflicts such as the Korean War (1950-1953), the Vietnam War (1955-1975), the Gulf War (1990-1991) and the wars in Afghanistan (2001-2021) and Iraq (2003-2011). According to Manring et al’s 2009 historical review, “Trauma care for US soldiers in Iraq and Afghanistan currently is provided through five levels of care: Level I, front line first aid; Level II, FST (Forward Surgical Team); Level III, CSH, which is similar to civilian trauma centers; Level IV, surgical hospitals outside the combat zone…and Level V, major US military hospitals…” (Manring et al., 2009, pg. 2171)
Photo and caption via National Archives Catalog. Caption: An aerial view of a field hospital erected during Exercise WOUNDED EAGLE '83.
The path to our current military medicine field and system was windy. The field was influenced by scientific advances and historical figures such as Baron Dominique-Jean Larrey, Florence Nightingale, Dr. Walter Reed, Leonard Wood and thousands of physicians, surgeons, nurses, ambulance drivers and other professionals. If you are interested in hearing firsthand accounts from military healthcare professionals, visit the Library of Congress’ collection ‘Healing with Honor: Medical Personnel.’ The collection features personal narratives from people who served in conflicts such as World War I, the Korean War or the war in Afghanistan. ‘Healing with Honor: Medical Personnel’ is an excellent way to learn more about the field of military medicine and its commitment to the treatment of soldiers harmed during conflicts.
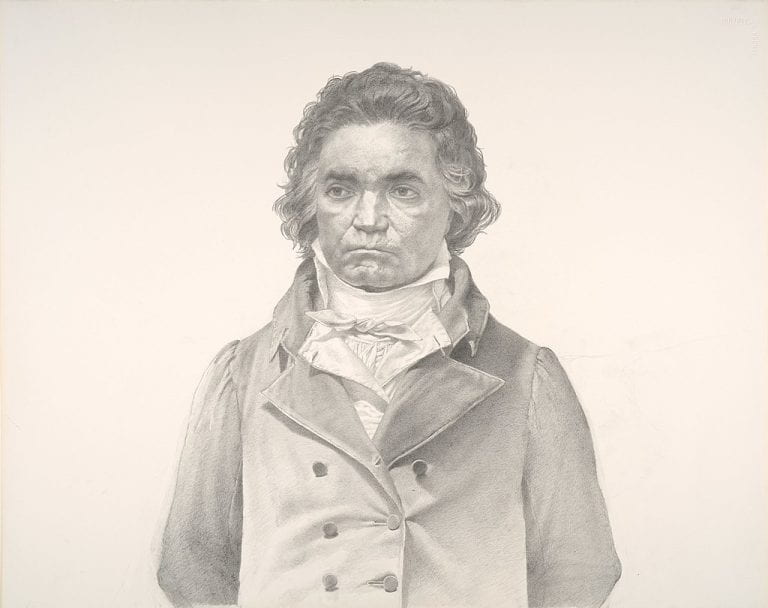
Scott Gentling (1942-2011).Beethoven.[undated].Graphite on paper.Amon Carter Museum of American Art, Fort Worth, Texas.2018.70, CC BY-SA 4.0, via Wikimedia Commons
Beethoven, one of the great musical geniuses of the 19th century, was deaf when he wrote some of his best known works. He had progressive hearing loss starting in his 20’s and was functionally deaf during his late period when he wrote his most expressive and innovative sonatas, string quartets, and the Ninth Symphony (Ode to Joy). Beethoven also suffered from gastrointestinal symptoms most of his adult life and died of liver failure. In 1802, he requested that his medical conditions be disclosed to the public after his death in a letter to his brothers known as the Heiligenstadt Testament.
Historians and musicologists have speculated if he had a heritable disorder or infectious disease that contributed to his hearing loss and death. Alcoholism was suspected as a factor in his liver disease. There was a family history of alcohol dependence and some of his associates claimed he drank heavily, though others said he did not drink more than was typical at that time.
Recent advances in ancient DNA methods presented an opportunity to learn more about Beethoven’s medical conditions. A team of 32 international researchers used eight surviving locks of Beethoven’s hair for their analysis. Several locks were taken by friends when Beethoven died in 1827 and others were given to friends and associates while he was alive. Over the years they were sold and passed down to others and the provenance of some were questionable. The locks were analyzed in this new study to determine their authenticity, using a novel geo-genetic triangulation technique. Additionally, the researchers “analyzed Beethoven’s genome for genetic causes of and risk for somatic disorders in addition to metagenomic screening for evidence of infections, followed by targeted DNA capture.” (Begg, et al, 2023)
Five of the locks were determined to originate from a single individual or monozygotic twins and had damage patterns that authenticated them for early 19th century origin. A non-matching lock called the Hiller lock was used in previous genetic and forensic testing featured in the book and movie, Beethoven’s Hair. It was found to be from a woman, invalidating results indicating lead poisoning as a contributor to Beethoven’s hearing loss and other maladies.
Analysis on the Y chromosome revealed a surprise finding. Five living men from the Beethoven patrilineage had a common ancestor in Aert van Beethoven (1535-1609). But their Y chromosomes did not match with any of the five authenticated Beethoven hair samples. The researchers conclude that there was at least one extra pair paternity event in Beethoven’s ancestry. Further analysis of descendants of Beethoven’s brother Karl leaves open the possibility that the two may have been half brothers.
Beethoven’s GI symptoms were consistent with Crohn’s disease or ulcerative colitis. His hearing loss could have been associated. Other possible related causes for the hearing loss were otosclerosis, sarcoidosis or systemic lupus erythematosus. A genome wide association study eliminated most of these as possibilities, except for lupus where there was some elevated polygenic risk.
Celiac disease and lactose intolerance were both eliminated as possible causes of his gastrointestinal symptoms through testing for associated alleles. He actually had some elevated genetic protections against irritable bowel syndrome, making it also unlikely.
They analyzed 55 genes where variants could cause monogenic post-lingual hearing loss and 209 related to pre-lingual hearing loss. There were no positive findings.
In summary, we could not reliably evaluate most hypothesized multifactorial causes of Beethoven’s hearing loss, nor did we identify a monogenic origin.”
(Begg, et al, 2023)
Beethoven’s polygenic risk for liver cirrhosis was found to be elevated in his PNPLA3 gene and his HFE gene. This combined with heavy drinking could have caused his liver failure. Additionally, hepatitis B DNA was found in the Stumpff Lock hair which was the best preserved sample. Researchers could not tell how long he’d had the hepatitis B infection. The positive lock was taken at his death and represented the final months of his life. Tristan Begg, the lead author of the study, wrote more about the possible role of hepatitis B in Beethoven’s liver failure on William Meredith’s blog. Meredith is a Beethoven scholar who participated in the genome study.
Though not addressed directly in the paper, the study brings to an end the theory that Beethoven was black. Noting the similarities in their appearance, the bi-racial composer Samuel Coleridge-Taylor was the first to raise the possibility. Many contemporaries of Beethoven described him as dark, brown or ruddy in complexion and noted his broad, rounded nose which can be seen in his life mask taken in 1812. The idea has persisted since Coleridge-Taylor introduced it, and was repeated by Malcolm X and a 1969 Rolling Stones article titled “Beethoven was black and proud!” More recently it was the subject of scholarly articles and even a Twitter meme. This genomic analysis confirms that Beethoven’s ancestry was greater than 99% European, with the strongest autosomal match with present day North Rhine-Westphalia in Germany.
Although there was no definitive finding on Beethoven’s hearing loss, there was plenty to advance the existing knowledge base and establish leads for future research. The study demonstrates how much can be learned from a few strands of centuries old hair through new genetic analysis tools.
References
Begg TJA, Schmidt A, Kocher A, et al. Genomic analyses of hair from Ludwig van Beethoven. Curr Biol. 2023 Apr 24;33(8):1431-1447.e22. doi: 10.1016/j.cub.2023.02.041. Epub 2023 Mar 22. PMID: 36958333.
Photo: Jose Ramon Pato from Coruña, España, CC BY-SA 2.0, via Wikimedia Commons.
If you’ve watched the hit show The Last of Us, you probably know about the “zombie fungus” cordyceps and would prefer to avoid it like the plague. Cordyceps is actually a highly coveted ingredient in traditional Chinese medicine. But what is it? And could this “zombie fungus” actually be useful in treating certain medical conditions?
Cordyceps is a fungus parasite that typically lives on caterpillars and other insects in the mountains of China (Natural Medicines, 2023b). To grow, cordyceps attach to a host, often a caterpillar, and the fungus root structure (mycelia) eventually spread throughout the host’s body, until the fungus has taken over the host’s tissue completely, thus killing the host (Natural Medicines, 2023a). The Last of Us portrays cordyceps as prevalent in the wild, but it’s actually pretty hard to find. So difficult to find in the wild, that the cordyceps that end up in commercial products (including dietary supplements with purported “anti-aging” benefits) are grown and fermented in a lab (Natural Medicines, 2023a).
While Cordyceps does “induce zombielike symptoms in insects” (Hume, 2023), it might help improve immunity and have positive effects on cancer and tumor size (Natural Medicines, 2023a). There is currently a lack of large, randomized controlled clinical trials on the use of cordyceps, which makes it difficult to make definitive statements about its efficacy (Lexicomp, 2020). However, it has been used in doses of 3-6 grams daily for up to one year with apparent safety (Natural Medicines, 2023b).
Cordyceps had traditionally been used to “improve weakness, impotence, and fatigue associated with aging” in elderly populations (Lexicomp, 2020). It has also been shown to produce modest improvements in biomarkers in some patients with chronic kidney disease (CKD), as well as modestly improve COPD symptoms (Natural Medicines, 2023b). However, it’s important to note that the studies that produced these results were small clinical studies and that further research is needed. Cordyceps has also historically been used to treat heart disease, showing improvement in cardiac function, arrhythmias, and overall quality of life (Lexicomp, 2020). Again, it’s important to note that these results have not yet been confirmed by large, high-quality clinical trials (Lexicomp, 2020).
While cordyceps is enjoying a resurgence in popularity and is being discussed more widely thanks to the popularity of The Last of Us, more research is needed to determine if it has safe and effective medicinal uses, and there has yet to be any sound scientific evidence that supports it use (Natural Medicines, 2023a). However, perhaps its recent popularity will result in further research on cordyceps and its potential uses.
Are you interested in examining how health and other news is being reported to television audiences? Are you interested in gaining a historical perspective on health topics through broadcast news? The Vanderbilt Television News Archive is a unique resource to help you do this.
Streaming content is available from CNN and NBC.
The archive, housed at Vanderbilt University, has been recording and indexing national nightly news broadcasts from the United States since August 5, 1968. Initially the news broadcasts recorded included only the “big three” networks, ABC, CBS, and NBC. With the creation of CNN and Fox News, additional news content was added to the archive. Broadcasts are indexed and made keyword searchable.
While not all news networks provide their streaming content to the archive, Vanderbilt has been able to reach agreements with two networks, CNN and NBC, to provide streaming content within the archive’s web interface. Where streaming video is available, there will be a link to play the content.
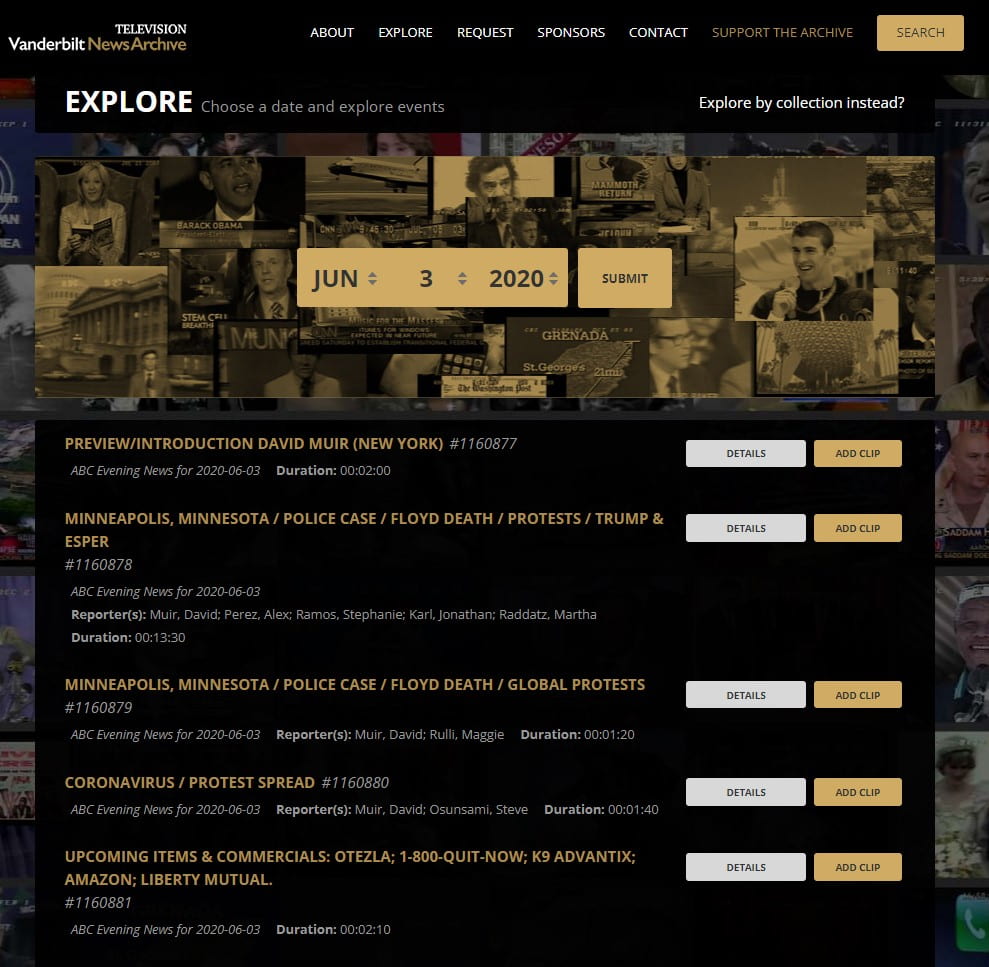
You can search the archive by browsing for news from a particular date, going as far back as August 1968. Browsing by date reveals summaries of all the segments within that day’s broadcasts from all available networks. The summary shows the topic of the segment, its length, and lists the reporters for that segment.
Browsing the archive by a specific date is one option.
Another interesting feature of the broadcast summary is that it details which products (including medications) were advertised during commercial breaks. Where streaming content is available, you can view those advertisements.
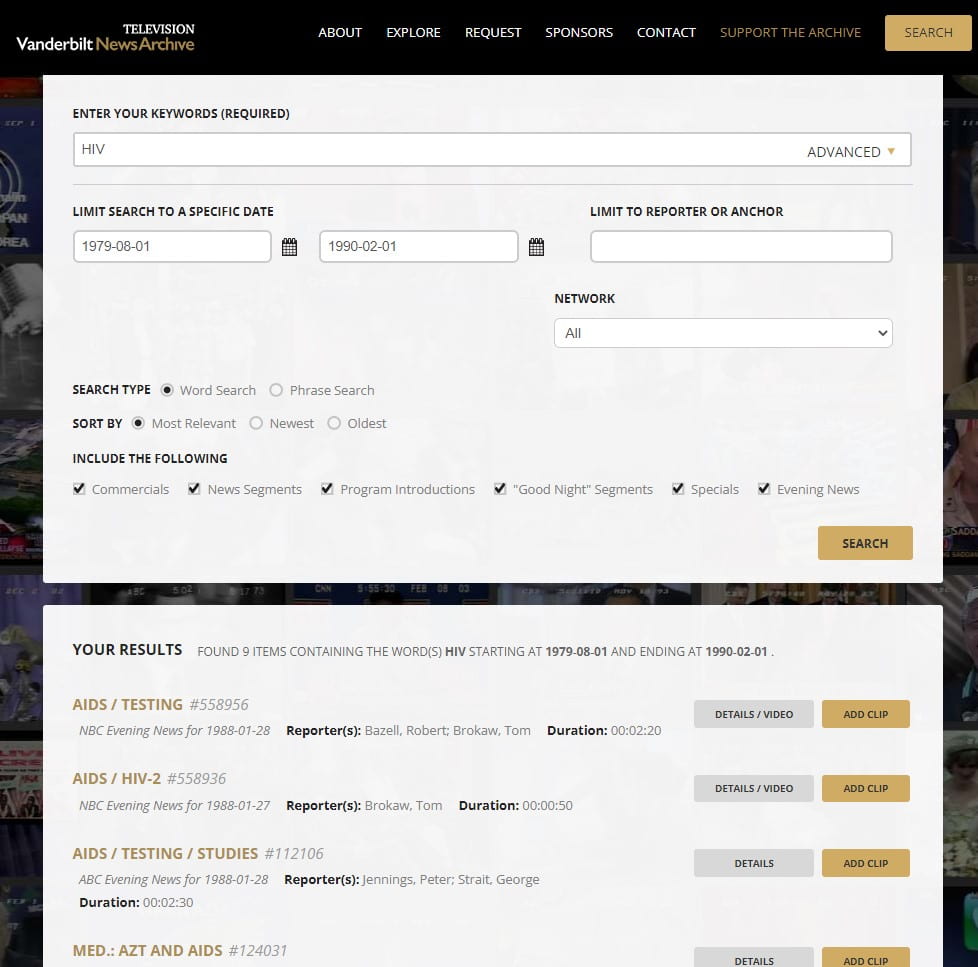
You can also search by keyword to produce a list of broadcast segments with relevant content, limiting by date range if desired:
Keyword searching the archive is another option.
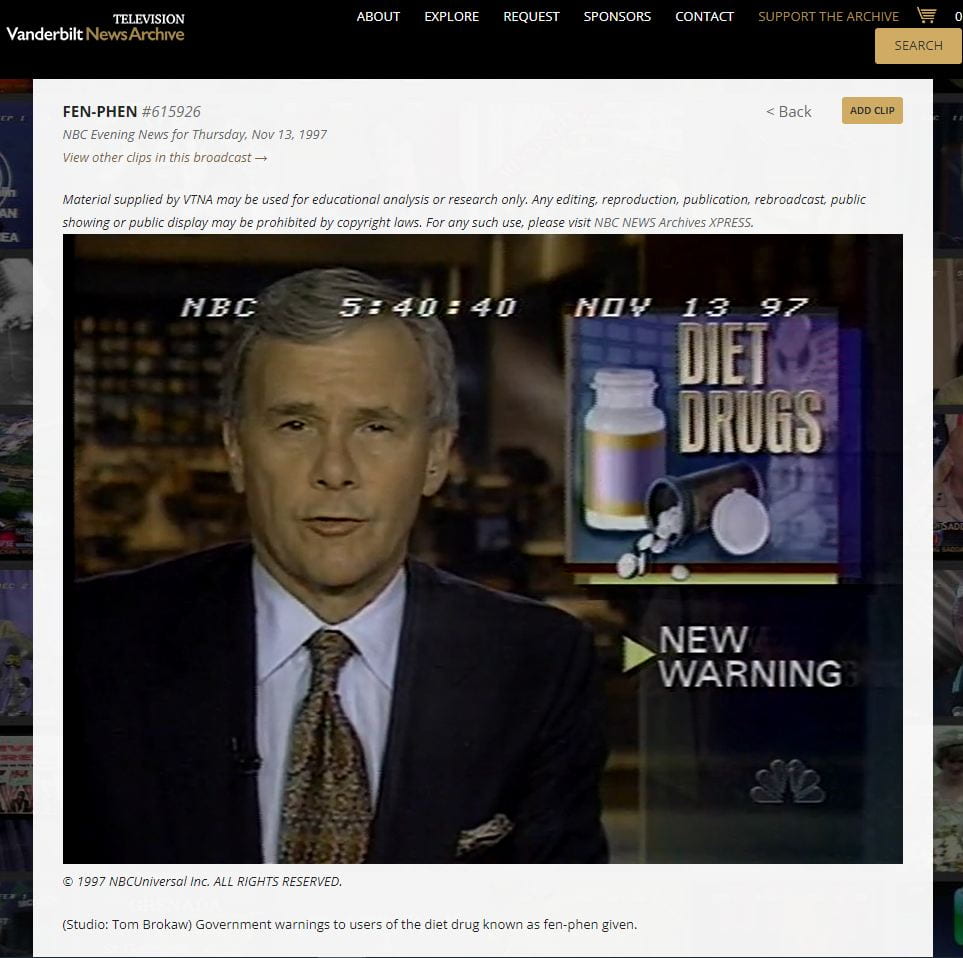
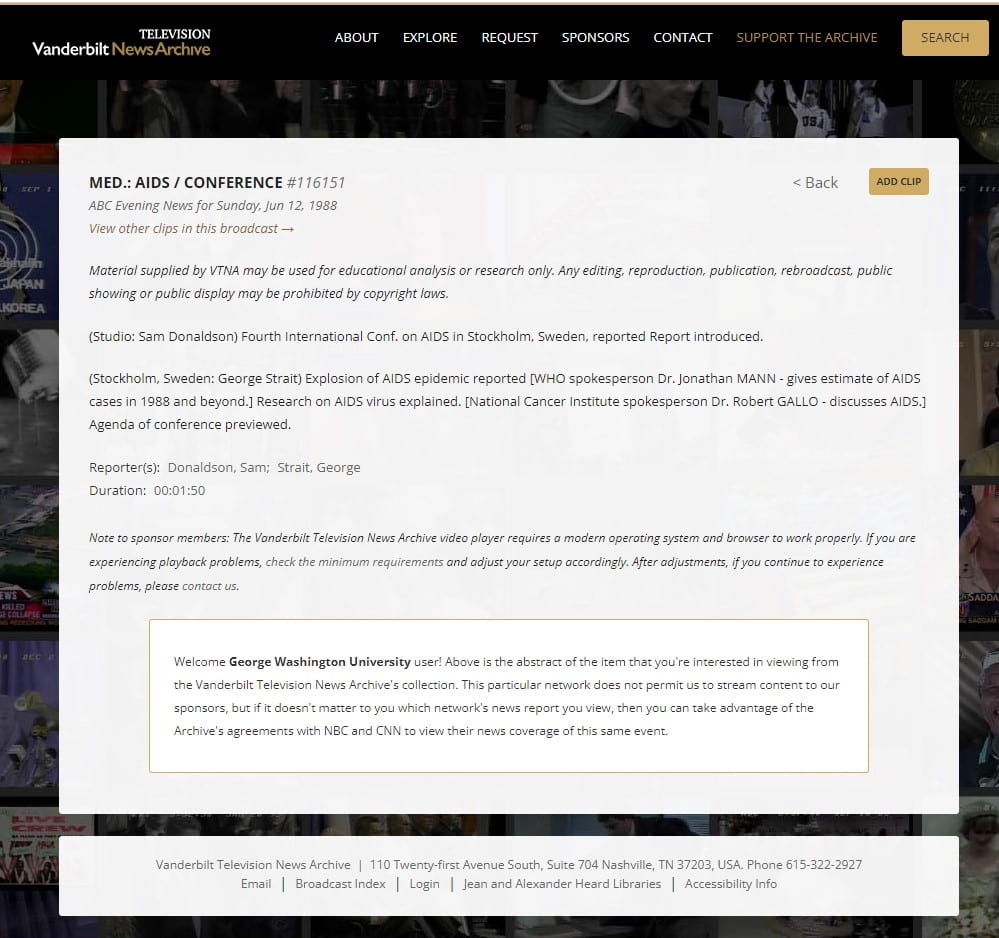
For networks from which only an abstract of a broadcast is available, the information provided is robust enough to establish the content of the report, its length, and the interviews included:
Even when streaming content is unavailable, each segment is described in detail.
The Vanderbilt Television News Archive is a fascinating way to watch the evolution of health topics and other issues and events over time. This unique resource lets you explore, for example, the way in which HIV/AIDS was discussed in the earliest newscasts on the subject; trace media coverage of the beginning of the COVID-19 pandemic, either via keyword search or browsing broadcasts by date; examine changes in the way medications were advertised on national television; and so much more.
Access to clips from the archive which are not available for streaming are generally assessed a loan fee, with full details available on the Request page. However, researchers located in the Washington, DC area can access full streaming content from the archive at the Library of Congress Moving Image Research Center. Appointments to use the facility are required, and can be made here.
2023 marks the 52nd anniversary of the National Blood Donor Month! This is a perfect time to understand the many benefits of donating blood, especially during the months when it is most critically needed. Currently, hospitals stand at concerning levels with regards to blood supply.
January is well known for being a time of self reflection & change, and a time where we make goals centered around what we desire to accomplish in life. What better way to support not only ourselves, but each other by making a contribution to the many who are in need? All types are accepted, and type O is needed the most.
To make an appointment to donate, contact the American Red Cross by using the Red Cross Blood Donor App, by visiting RedCrossBlood.org or calling 1-800-RED CROSS (1-800-733-2767).Those who have received Moderna or Pfizer COVID vaccines are eligible to donate without wait. Remember, a donation is not simply a donation, but also an action which can help save lives.
To learn more about the importance of blood donation, visit the Association for the Advancement for Blood & Biotherapies website to learn about blood as an essential medicine and about how our community is making an effort to drive donor diversity. Also, donating blood is also a way to receive a free health screening? Some underlying health conditions such as genetic mutations or hereditary hemochromatosis can be found simply by donating blood.
Lastly, did you know that the School of Medicine and Health Sciences actually has a Post-Baccalaureate Certificate in Blood Banking for Medical Laboratory Science? To find more about this online program, its career outlook and curriculum, we highly recommend that you request more information to see if this is the right course for you.












{kind=link}