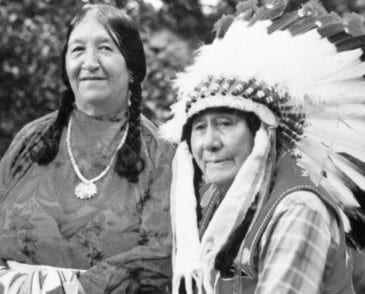
Susie Walking Bear Yellowtail (Women's History Matters)
In an effort to remain accountable to communities who have been negatively impacted by past and present medical injustices, the staff at Himmelfarb Library is committed to the work of maintaining an anti-discriminatory practice. We will uplift and highlight diverse stories throughout the year, and not shy away from difficult conversations necessary for health sciences education. To help fulfill this mission, today's blog post examines the life and activism of Susie Walking Bear Yellowtail.
Susie Walking Bear Yellowtail was a Native American nurse who consistently advocated for better access to quality, culturally sensitive healthcare and during her decades long medical career, she documented and recounted stories of medical abuse that Native Americans frequently experienced when visiting hospitals or non-Native doctors. Yellowtail was one of the first Native American registered nurses and the first registered nurse from the Crow people. Her work as an activist paved the way for other medical professionals who sought to end harmful practices that frequently impacted lower-class families and people of color.
Yellowtail was born on January 27, 1903 on the Crow Indian Reservation in Montana. She was orphaned at a young age, but lived with an aunt who took care of Yellowtail and her sister. Like many young Native children, Susie Yellowtail attended an Indian boarding school until she met the Baptist missionary, Frances Shaw. Yellowtail traveled with Shaw to a Baptist convention in Denver, before moving to Oklahoma to complete her education at the Bacone Indian School. When Frances Shaw married and became Mrs. Clifford Fields, Yellowtail once again moved to the East where she lived with the Fields family. During this time, Susie Yellowtail enrolled in Northfield Seminary. Mrs. Fields paid for the tuition fees, but to afford her room and board, Yellowtail worked as a nanny and maid for the Fields family. Eventually she left the seminary and instead enrolled in a nursing program at Franklin County Memorial Hospital and completed her training at the Boston City Hospital School of Nursing. She received her degree in 1927 and worked in several different positions before returning to the reservation where she was born.
Working as a nurse for the Indian Health Service’s run hospital, Yellowtail witnessed firsthand the mistreatment many Crow people experienced during their appointments. She “documented instances of Indian children dying from lack of access to medical care, Indian women being sterilized without consent, and tribal elders unable to communicate their health concerns to doctors.” (Women's History Matters) Yellowtail sought to provide better treatment for her community and was vocal with her criticisms of the non-Native doctors, nurses and medical professionals who worked in the hospital. She blended her Crow culture and traditions with her medical education to care for Native patients who were nervous around the hospital staff or unable to access the hospital and its services. In 1929, Susie Walking Bear married Thomas Yellowtail and the two became major leaders on the reservation.
Thomas and Susie Yellowtail (Women's History Matters)
Susie Walking Bear Yellowtail served as a member of several reservation advisory committees and this eventually led to President John F. Kennedy appointing her to the Surgeon General’s Advisory Committee on Indian Health. She was reappointed to this position by both the Johnson and Nixon administrations. In this role, Yellowtail traveled to other Native American reservations and documented Native Americans’ experiences with visiting their hospitals. Almost immediately, she noticed a similarity in stories and used this information to create recommendations that would improve not only the relationship between Native Americans and health professionals, but also address years of harm that went unchecked. Susie Yellowtail continued her work for decades and died on December 25, 1981.
Yellowtail received recognition for her work both during her lifetime and after her passing. She was awarded the President’s Award for Outstanding Nursing by President Kennedy in 1962 and she was inducted into the Montana Hall of Fame in 1987. In 2002, she was also inducted into the American Nurses Association Hall of Fame.
While Susie Walking Bear Yellowtails’ career and advocacy efforts positively impacted the Crow people and other Native American tribes in her lifetime, her work served as an example on how health rights activists could monitor and document patient mistreatment by the medical field. Yellowtail used her Crow identity and nursing education to provide culturally sensitive care to the Native Americans who requested her services. As one of the first registered nurses of Native American descent, Susie Yellowtail embedded herself in the medical field and brought about long-lasting changes that can still be felt to this day.
In an effort to remain accountable to communities who have been negatively impacted by past and present medical injustices, the staff at Himmelfarb Library is committed to the work of maintaining an anti-discriminatory practice. We will uplift and highlight diverse stories throughout the year, and not shy away from difficult conversations necessary for health sciences education. To help fulfill this mission, today's blog post highlights/celebrates National Native American Heritage Month.
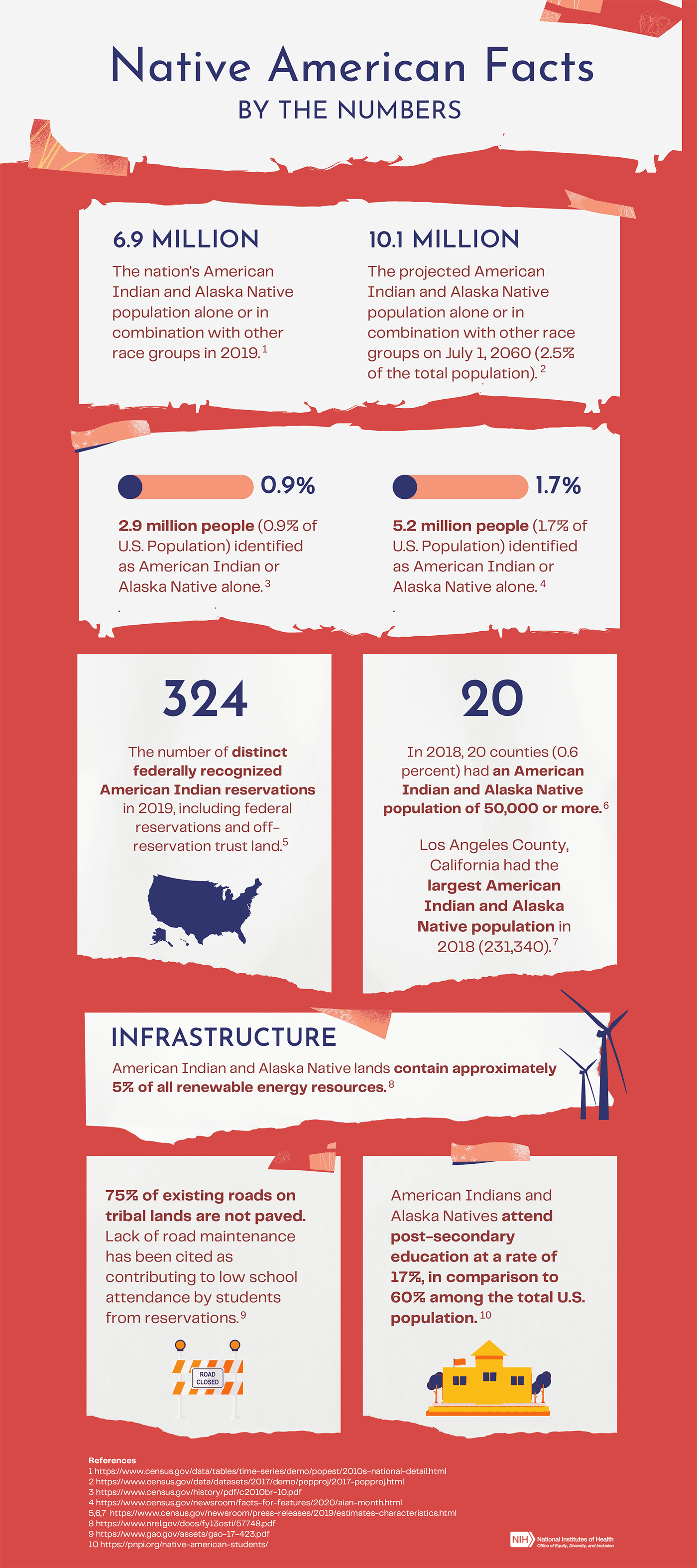
For November’s National Native American Heritage month, there are many ways to spread appreciation and promote equality and diversity in your own area. The NIH has prepared events and a useful infographic along with several blog posts to celebrate and educate about the achievements and resources available to our Native American friends.
On November 16th, the NIH is also hosting a chat to explore internships and job opportunities in the field of Medicine. Even if you are already employed it can be helpful to gain some insight from Native professionals who are able to offer advice and career highlights! This is an interactive virtual discussion so you will be allowed to ask questions and converse with the panelists directly! Find out more information about the event at the NIH Website.
Additionally, the Smithsonian will be hosting a Native Cinema Showcase as a celebration of the best in Native film. This year’s focus is on highlighting Native people who have boldly asserted themselves through language, healing, building community, and a continued relationship with the land. Each film will be available on Demand through the Smithsonian’s Cinema Showcase page, and we definitely recommend checking out a film or two!
Looking to de-stress? How about spending an afternoon with a good book or some poetry written by the current US poet Laureate is Joy Haro, the first Native to earn the title.
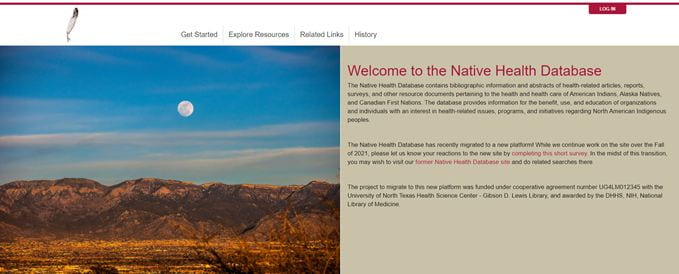
In an effort to remain accountable to communities who have been negatively impacted by past and present medical injustices, the staff at Himmelfarb Library is committed to the work of maintaining an anti-discriminatory practice. We will uplift and highlight diverse stories throughout the year, and not shy away from difficult conversations necessary for health sciences education. To help fulfill this mission, today's post will highlight the Native Health Database.
The Native Health Database is an online collection that organizes and shares information related to the health and health care of American Indians, Alaska Natives and Canadian First Nations. The Native Health Database “...provides information for the benefit, use, and education of organizations and individuals with an interest in health-related issues, programs and initiatives regarding North American Indigenous peoples.”
Created in the 1990s, the Native Health Database is the final result of the merging of two different Native American health care collections, the Native Health History Database and the Native Health Research Database. When Dr. William W. Schottstaedt donated over 3,000 documents to the University of New Mexico’s Health Sciences Library and Informatics Center, the resources were compiled into the Native Health History Database. The historical documents dated from 1672 to 1966 and were collected into a single database that focused on the history of health and healthcare of Native American people.
The Native Health Research Database began in 1997 when the United States Indian Health Service contracted with The Health Sciences Library and Informatics Center to create a resource that covered the current landscape of Native American health. These two databases merged into the Native Health Database in 2007, and recently transitioned to the Mukurtu CMS platform with the goal of giving Native American groups and individuals better control and access to the content that’s available for viewing and sharing.
The Native Health Database does not require users to create an account to browse or access items in the collection, but registered users can save items to their personal collection for later review and registration is free.
When searching for a resource, you can refine your search by the date, tribal or group affiliation, subject, resource type or by other parameters. Resource types include, but are not limited to, journal articles, editorials, guidelines and monographs. While the full resource is not stored on the database, the individual database records provide information to guide you to the manuscript or document elsewhere.
You may use the item’s identifier to search for the resource through an external link such as PubMed Central. If you’re interested in the physical copy of the resource, you can contact the Native Health Database administrator at hsc-nhd@salud.unm.edu to request access to the resource. Please note these requests are granted on a case-by-case basis.
The Native Health Database is an excellent resource for learning about the historical and current needs of Native American communities. With documents ranging from the late 1600s to now, the database covers a broad spectrum of topics and time periods. The content available through the Native Health Database is meant to serve as a springboard for individuals as they explore the specific topics and needs that directly impact Native American groups. By increasing their level of understanding of Native American health, medical professionals and researchers will have the ability to better address the needs of their patients or undertake research opportunities that are respectful of Native American people and communities.
Today we would like to highlight just a few of the many men and women who have changed the health sciences professions.
Ildaura Murillo-Rohde, PhD, RN (1920-2010): Changing the face of nursing
Ildaura Murillo-Rohde who, after witnessing many hispanic communities being treated by mostly non-hispanic providers, was dismayed at what she saw. Determined to change this,, she created the National Association of Hispanic Nurses (NAHN) in 1975.
“I saw that I was the only Hispanic nurse who was going to Washington to work with the federal government, review research and education grants, etc.,” Murillo-Rohde later noted. “I looked behind me and thought: ‘Where are my people?’”
Not only did she create the National Association of Hispanic Nurses, Dr. Rodhe was also the first Hispanic dean of nursing at NYU. Read more about Dr. Rohde’s accomplishments:
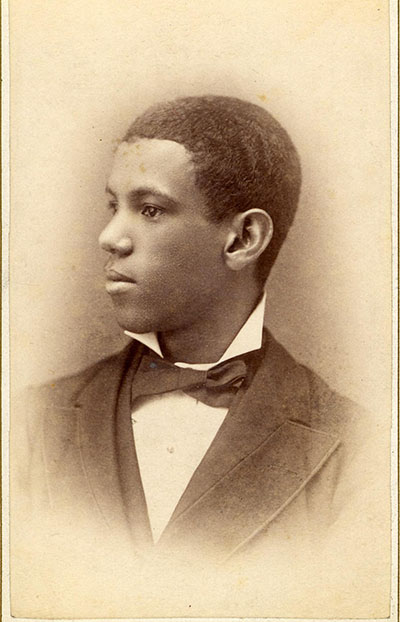
José Celso Barbosa, MD (1857-1921): the “father of the Puerto Rican statehood movement.”
José Celso Barbosa was no stranger to discrimination. Despite this, his determination did not falter in his attempts to help others.
In 1875, Barbosa left his home of Puerto Rico to New York City. After a brush with pneumonia, he became interested in the field of medicine. Unfortunately, university officials rejected his application, stating that they would not accept students of color.
Undeterred, Barbosa graduated from the University of Michigan as the first Puerto Rican to receive a Medical degree in the United States.
He continued to care for soldiers during the Spanish - American war and through the Red Cross he was able to treat many poor patients in Puerto Rico. He articulated that there was a need for employer based health care insurance, which was a radical idea at the time.
Later in his career, Barbosa founded a party that urged U.S. statehood for Puerto Rico. For that leadership, Barbosa has been dubbed the “father of the Puerto Rican statehood movement.” Read more about Dr. Barbosa’s accomplishments:
In Washington D.C. and across the country today is Indigenous People’s Day, a holiday that recognizes, honors and celebrates Indigenous people, cultures and history.
Indigenous Peoples’ Day was first proposed in 1977 during the United Nations International Conference Discrimination against Indigenous People in the Americas. “Indigenous Peoples’ Day recognizes that Native people are the first inhabitants of the Americas, including the lands that later became the United States of America. And it urges Americans to rethink history.” The first state to adopt Indigenous Peoples’ Day as a recognized holiday was South Dakota in 1990 and since then more states have replaced Columbus Day with Indigenous Peoples’ Day or celebrate the two holidays together. The movement to celebrate Indigenous Peoples’ Day is still ongoing as more states, towns and localities draft and adopt resolutions to recognize this holiday in lieu of Columbus Day. On October 8th, 2021, President Biden signed a proclamation in honor of Indigenous Peoples’ Day 2021, stating “On Indigenous Peoples’ Day, our Nation celebrates the invaluable contributions and resilience of Indigenous peoples, recognizes their inherent sovereignty, and commits to honoring the Federal Government’s trust and treaty obligations to Tribal Nations.”
As Indigenous Peoples’ Day becomes more widely recognized across the country, many states and towns hold educational and celebratory events where people can learn more about Indigenous people and tribes. Here are a few ways in which you can observe Indigenous Peoples’ Day this year:
Read a book written by an Indigenous author- The list of published books, articles and other sources written by Indigenous people grows longer every year. “An Indigenous Peoples’ History of the United States” and it’s companion book “An Indigenous Peoples’ History of the United States for Young People” are texts that offer a different perspective on the pre- and post-colonial Americas. The books also offer a list of citations and sources at the end if you’re interested in learning more about a specific period or topic in Indigenous history. If you’re interested in reading Indigenous fiction, check out “Black Sun” by Rebecca Roanhorse, “There, There” by Tommy Orange, or select a book from Penguin Random House’s list of “Must-Read Books by Indigenous Authors”.
Learn about Indigenous history and culture- There are two branches for the National Museum of the American Indian, one in Washington D.C., while the other is in New York. The D.C. location is open Wednesdays-Sundays from 10 am-5:30 pm. But if you’re unable to visit the physical location, the museum’s website offers virtual exhibits and educational resources. Start with the handout ‘Unlearning Columbus Day Myths’ or explore the Native Knowledge 360 learning module, which helps students and educators examine their approach to learning and understanding Native history. You can also search their collection with their online database. The virtual collection is divided into several different categories to help you refine your search or explore at your own pace and see if you come across a fascinating new piece of information.
Indigenous Peoples’ Day is a great opportunity to reflect on a new perspective to American history. It is also a time to think about Indigenous futures and how Indigenous culture impacts our society. No matter how you decide to celebrate Indigenous Peoples' Day, recognize that learning history from a different point of view is one step in which we can create a more equitable and fair environment for all.
In an effort to remain accountable to communities who have been negatively impacted by past and present medical injustices, the staff at Himmelfarb Library is committed to the work of maintaining an anti-discriminatory practice. We will uplift and highlight diverse stories throughout the year, and not shy away from difficult conversations necessary for health sciences education. To help fulfill this mission, we’re proud to reach out to one of our own Faculty members, Dr. Carlos Rodriguez-Diaz to hear his perspective on the COVID-19 vaccine, and what made his journey to the field of public health truly unique.
What inspired you to go into public health? How did you first get involved in HIV care and prevention?
I was inspired to pursue a career in public health by a family physician who was by head physician and was the primary health care provider to my family and almost everyone in the small town of Aguas Buenas, Puerto Rico where I was born and raised. Before my senior year in college, I had the opportunity to participate in a Summer Internship Program at the University of Michigan-School of Public Health. I had the opportunity to work with a Latino-serving organization and it was through this experience that I got involved in public health and HIV prevention. Then, I realized the privilege that I had as a young Latino gay man to have access to education and contribute to my community by engaging in public health training, practice, and research. I am now using my privilege to disrupt privileges.
What brought you to GW?
After nearly a decade working at the University of Puerto Rico-School of Public Health, I felt it was the time to expand my experiences and contribute to public health efforts in Puerto Rico but from a different platform. I also wanted to be more engaged in public health initiatives at US national level. GW’s location in the US capitol was a very attractive, particularly after experiencing at first had how public health efforts in the US are hindered by the lack of representation and the colonial experience of Puerto Rico. Further, GW is an established institution with ample experience conducting research in areas of my interest and expertise.
What has been the most rewarding aspect of your work?
The opportunity to work with community members to identify public health challenges and address these challenges.
We see a rise in misinformation with the COVID-19 vaccine. What lessons do you think scientists and medical experts can learn from that? How can scientific research be more transparent and accessible to the public?
We need to listen and to be better communicators. Based on my experience, most of the questions people have about the COVID-19 vaccine are legitimate. People need to be listened to and must receive culturally appropriate information. As scientists, we need to work on our health communications skills. We might be experts in an area of knowledge, but that does not mean that we know how to communicate information to lay populations. We either develop skills to engage with multiple audiences or work with experts who can help us communicate effectively. Further, we should facilitate those scientists from minoritized populations (e.g., Latinos, Black, LGBTQ, Native Americans) to have access to mass media and platforms to reach out to their communities. No one else can speak to a community like a community member.
What are your future research related plans or areas of interest at this time?
I plan to continue working with community-based organizations and other community leaders to develop strategies to reduce health inequities and health disparities. The beauty of conducting community-based participatory research is that we are constantly focusing on the priorities identified by the community rather than working on a rigid research agenda. I also expect to continue my engagement in research activities related to the Ending the HIV Epidemic. I am collaborating in community-centered projects to address social determinants of HIV in Washington, DC and Puerto Rico. I am also planning to continue to be engaged in COVID-19 related research with Latino populations.
We now have multiple vaccines for COVID and more are in development based on a wide variety of techniques. Do you see this progress as potentially helpful in the development of an HIV vaccine?
Yes. The SARS-CoV-2 vaccine effort organized extraordinary resources and unprecedented global collaborations. The scientific achievements of COVID-19 vaccines are now inspiring a renewed sense of urgency for the HIV vaccine development effort.
What advice, if any, do you have for students just starting out?
Aim for what you are passionate about. Always be yourself. Never become someone else to achieve your goals. Listen to your mentors and once you achieve your goals, pay it forward.
On behalf of the Himmelfarb library we would like to extend our thanks to Dr. Rodríguez-Díaz for participating in this interview!
In an effort to remain accountable to communities who have been negatively impacted by past and present medical injustices, the staff at Himmelfarb Library is committed to the work of maintaining an anti-discriminatory practice. We will uplift and highlight diverse stories throughout the year, and not shy away from difficult conversations necessary for health sciences education. To help fulfill this mission, today's blog post honors Dr. Helen Rodriguez Trias!
A pediatrician and women and children’s health advocate, Dr. Helen Rodriguez Trias deeply believed medical professionals must immerse themselves in the social issues impacting the communities they serve and wove this personal philosophy into her medical and advocacy work. Over the course of her career, she consistently spotlighted issues facing women and children, particularly those that were people of color, poor or disabled.
Dr. Helen Rodriguez Trias was born on July 7, 1929 in New York, though she spent the first few years of her life in Puerto Rico with her family. Upon her return to the United States, she faced racial discrimination while attending public school. Despite receiving good grades and her use of English, Dr. Rodriguez Trias was placed in special education classes. She remained in this setting until she recited a poem by heart and her teacher realized Rodriguez Trias was placed in the wrong class.
After completing high school, Dr. Rodriguez-Trias returned to Puerto Rico for college. During her time as a student, she became involved with the island’s independence movement and participated in a school-wide strike against the university’s chancellor, Jaime Rexach Benitez, who prevented the Puerto Rican Nationalist Party leader, Don Pedro Albizu Campos, from speaking on campus. Because of her involvement in the strike, Dr. Rodriguez-Trias was forced to return to New York City when her brother threatened to cut her off financially. She remained in the United States for several years before returning to the University of Puerto Rico, where she eventually graduated with a BA in 1957 and her medical degree in 1960.
Not long into her medical career, Dr. Rodriguez-Trias worked to address a major need within her immediate community. She established a newborn care clinic in the hospital and under her leadership, Puerto Rico experienced a 50% decrease in newborn mortality rates within the first 3 years of the clinic’s establishment. After completing her residency, she opened a pediatric practice in Puerto Rico and remained there until the 1970s.
At the time, Dr. Rodriguez-Trias was married, but divorced her husband before relocating to the United States. She often cited her divorce as a moment that deeply impacted her on a personal and professional level. "A watershed in my life was getting divorced in Puerto Rico....In my formation as a professional, there was always a kind of pressure to deny or not use a lot of your personal experience....But I was now discovering a whole other world out there through my personal experience of a deceptive marriage. That triggered quite a bit of growth in me toward understanding what happens internally to people, what happens in their lives and what they can do or not do...." (U.S. National Library of Medicine)
That experience would influence her for the rest of her career.
During the 1970s, Dr. Rodriguez Trias worked as the head of the pediatrics department at the Lincoln Hospital in the South Bronx. This was a diverse corner of New York with communities from all areas of the globe, including a large Puerto Rican population. During her tenure, Dr. Rodriguez Trias advocated for hospital employees to have a voice in administrative and patient-care issues. She frequently embedded herself in community conversations and encouraged the hospital medical professionals to engage with the community as well, so the medical staff had a better understanding of how outside issues impacted patients’ health.
Around this time, Dr. Rodriguez Trias also became heavily involved in the women’s movement and the women’s health movement, particularly on issues related to abortion access and the reproductive health abuse certain groups of women face. “While many women chose the [sterilization] procedure, health authorities pressured many other--especially working-class and poor women--to agree to it or falsely told them that it was reversible. Similar programs targeted poorer Black women and girls in the American South." ("Dr. Helen Rodriguez Trias") To combat these issues, Dr. Rodriguez Trias formed both the Committee to End Sterilization Abuse and the Committee for Abortion Rights and Against Sterilization Abuse. She testified before the Department of Health, Education and Welfare, advocating for the need for and eventually drafting federal guidelines for the reproductive procedure. The new guidelines featured three key components. First, doctors were required to explain the procedure in language that was accessible and easy to understand. Second, patients were required to submit written consent. Lastly, there was a mandatory wait period between the submission of consent and the medical procedure.
Dr. Rodriguez Trias would continue to speak up for women and children and their access to healthcare for the remainder of her career. On January 8, 2001, President Bill Clinton awarded Dr. Rodriguez Trias with the Presidential Citizen’s Award in recognition of her advocacy work for women and children impacted by the HIV/AIDS epidemic. And in 2019, New York City commissioned a statue of Dr. Rodriguez Trias that will be placed near the location where Lincoln Hospital once stood.
Dr. Helen Rodriguez Trias' life and career serve as examples for medical professionals who wish to impact their patients' lives outside of the hospital or private practice. She dedicated her time and energy to stand alongside the communities who needed equitable access to care and recognized that many outside factors impacted a person's level of health.
Wilcox, Joyce. “The Face of Women’s Health: Helen Rodriguez-Trias.” American Journal of Public Health, vol. 92, no. 4, 2002, pp. 566–69, doi:10.2105/ajph.92.4.566.
This Monday, July 26, 2021, marked the 31st anniversary of the Americans with Disabilities Act. This landmark legislation literally and figuratively opened the doors for millions of Americans with disabilities to equal access to jobs, education, transportation, and recreation. While we are often reminded of physical access in the form of providing ramps for wheelchairs, accessible seating in theaters, provisions for service animals in stores and public transportation, and interpreters for the hearing impaired, just as important are accessibility initiatives in the online world.
GW has a Digital Accessibility policy and trainings to enable those who provide web services and other online resources to ensure that content is accessible and usable to everyone in the University community. These policies are centered around WCAG (Web Content Accessibility Guidelines) standards; among them are making color contrast strong enough to be perceived, ensuring that fonts are of sufficient size and readability, providing alt-text for images, and providing for assistive technologies that allow navigation of a website by voice.
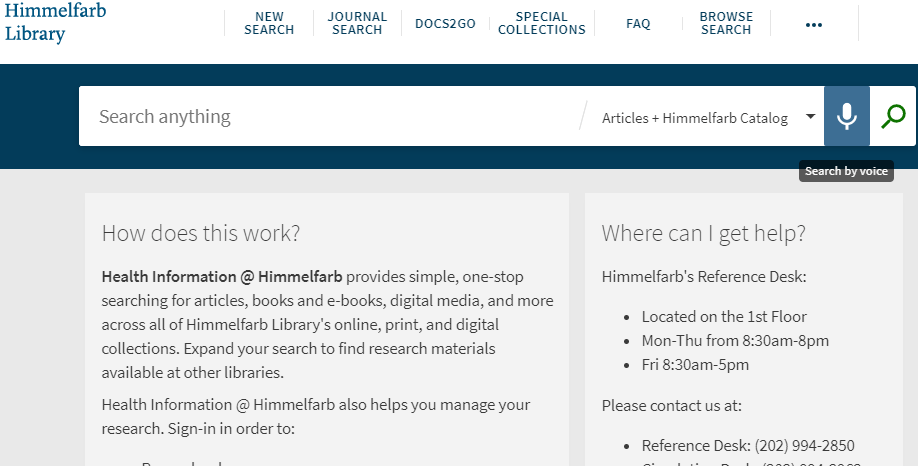
Recently the library’s search service, Health Information @ Himmelfarb, began providing a voice search component. Use the microphone icon next to the search bar to enable voice search.
In an effort to remain accountable to communities who have been negatively impacted by past and present medical injustices, the staff at Himmelfarb Library is committed to the work of maintaining an anti-discriminatory practice. We will uplift and highlight diverse stories throughout the year, and not shy away from difficult conversations necessary for health sciences education. To help fulfill this mission, today's blog post celebrates International Non-Binary Day!
July 14th is International Non-Binary Day! The first International Non-Binary Day took place in 2012 (Angulo, 2019). The date falls between International Women’s Day and International Men’s Day, making it an appropriate date on which to raise awareness of people who do not identify exclusively as man or woman. So what is non-binary?
Non-binary refers to anyone whose gender identity isn’t categorized as female or male. While some non-binary people identify as both a man and a woman, others don’t identify with either of these gender categories (HRC Staff, 2020). While some non-binary people identify as transgender, many do not. “Non-binary identities are varied and can include people who identify with some aspects of binary identities, while others reject them entirely” (Stonewall Staff, 2006). Simply put, being non-binary is as unique and individual as the people who identify as non-binary.
We can all be an ally to non-binary people. Some of the simplest things you can do to be inclusive involve being aware of how the language you use can have a positive impact on everyone, regardless of gender identity. Including your pronouns when you introduce yourself, in your email signatures and social media profiles can be a great starting point. When you introduce yourself, saying “Hi, my name is Jane and I use she/her pronouns” can be an easy way for other people to safely introduce their pronouns. This not only lets the person know that you are interested in using their correct pronouns, but also makes it easy for them to communicate their preferences to you if they wish. You may also consider using gender neutral language when you are addressing a group by replacing “ladies and gentleman” with “folks” or “everyone.” When mentioning relationships, consider using gender neutral terms such as parents (instead of father/mother), children (instead of sons/daughters), siblings (instead of brothers/sisters), or partner (instead of husband/wife, boyfriend/girlfriend).
From a medical and health perspective, non-binary people often experience health disparities resulting from their non-binary identities. One qualitative study published in 2020 in the Journal of Sex Research “explored the unique ways that non-binary adolescents experience minority stress and how it influences their mental health and well-being” (Johnson et al., 2020). Identity invalidation (the refusal to accept someone’s identity as “real” or “true”) was experienced during interpersonal relationships, within the LGBTQ communitity, on an institutional level in school environments, and through a lack of representation in the media (Johnson et al., 2020). The data collected from this study suggests that “identity invalidation has deleterious effects on mental health and contributes to mental health disparities facing non-binary adolescents” (Johnson et al. 2020).
A study published in the Journal of Health Care for the Poor and Underserved in 2018 examined interactions between transgender and gender non-binary individuals and their health care providers and identified characteristics of positive and negative interactions. Characteristics of positive clinician-patient interactions included: the correct use of names and pronouns; use of gender neutral language when referencing relationships, anatomy, and procedures; clinician knowledge of and experience with transgender and non-binary health; and treatment of identity disclosure as routine (Baldwin et al., 2018). Characteristics of negative clinician-patient interactions included: misgendering; lack of information and experience with transgender and non-binary patients (which often led to irrelevant questions stemming from clinician curiosity); and transphobia that led to a denial of care or a referral to another provider - another form of denial of care (Baldwin et al., 2018). This study concluded that formal medical education and training programs need to provide education and experience related to gender diverse patients. “Adjusting patient intake protocol and forms at the system-level to incorporate gender-neutral terminology and facilitate the use of preferred names and pronouns” was all supported by this study (Baldwin et al, 2018).
As we celebrate International Non-Binary Day this year, take some time to explore resources such as SMHS’s LGBTQIA+ Community Support page, and GW student groups such as GW Out for Health or Transgender and Non-Binary Students of GWU. One of the best ways to celebrate International Non-Binary Day is through education and learning more about the non-binary experience. The following video is a great starting point - take a look and learn what it’s like to be non-binary.
Baldwin, A., Dodge, B., Schick, V. R., Light, B., Scharrs, P. W., Herbenick, D., & Fortenberry, J. D. (2018). Transgender and Genderqueer Individuals’ Experiences with Health Care Providers: What’s Working, What’s Not, and Where Do We Go from Here? Journal of Health Care for the Poor and Underserved, 29(4), 1300–1318. https://doi.org/10.1353/hpu.2018.0097
Johnson, K. C., LeBlanc, A. J., Deardorff, J., & Bockting, W. O. (2020). Invalidation Experiences Among Non-Binary Adolescents. The Journal of Sex Research, 57(2), 222–233. https://doi.org/10.1080/00224499.2019.1608422
In an effort to remain accountable to communities who have been negatively impacted by past and present medical injustices, the staff at Himmelfarb Library is committed to the work of maintaining an anti-discriminatory practice. We will uplift and highlight diverse stories throughout the year, and not shy away from difficult conversations necessary for health sciences education. To help fulfill this mission, today's blog post features Dr. Lawrence “Bopper” Deyton, MSPH, MD.
Lawrence “Bopper” Deyton has been inspiring School of Medicine and Health Sciences (SMHS) students since March 2013 when he returned to SMHS after 31 years of government service at the Food and Drug Administration (FDA), the Department of Veterans Affairs (VA), the National Institutes of Health (NIH), Health and Human Services Office of the Surgeon General, and stints serving the Assistant Secretary of Health and as a Congressional Aide.
Deyton had an influential experience 46 years ago that “made me realize that massive education of the health and public health community needed to happen” (Roeder, 2019). The experience took place during a visit to the Harvard medical campus’ student health clinic for a sore throat while he was pursuing his Master in Public Health degree at Harvard. The physician who saw him for this complaint offered him a referral to a psychiatrist. After a moment's confusion, Deyton realized that the referral had nothing to do with his sore throat. “It was about me being gay” (Roeder, 2019). Having disclosed his sexual orientation on an intake form alongside answers to routine medical questions, he didn’t think it would be a barrier to obtaining medical care.
Rather than accept this experience as just the way life is, Deyton has been working to be a positive influence for change within health care his entire career. In his current role as Senior Associate Dean for Clinical Public Health and Murdock Head Professor of Medicine and Health Policy at SMHS, Deyton has been instrumental in creating the “Patients, Populations, and Systems” course which integrates concepts of public health, population health, health policy, advocacy and social responsibility with the clinical coursework in an effort to create “clinician citizens.” Deyton says “We want [students] to understand social determinants of health and to take up the mantle of their own social responsibilities when they leave here, and how what they learn here at GW can be used to effect positive social change” (Dvorak, 2018).
“Bopper,” a childhood nickname he has gone by his entire life and his first spoken word, had already been developing a deep sense of social responsibility as an undergraduate student. While pursuing his bachelor’s degree at the University of Kansas in the early 1970’s, Deyton remembers seeing a “Gay is good - Stonewall” poster and making the connection that “there was something out there that would allow me to integrate my sexuality with something that was positive” (Andriote, 1999). By the time he was pursuing his Master of Science in Public Health degree at Harvard, Deyton was doing exactly that. Even before his visit to the doctor about his sore throat, he had already become active in the American Public Health Association’s (APHA) LGBTQ Caucus, which was formed to help “tackle stigma in health care” (Roeder, 2019).
After moving to Washington, D.C. to work as a health policy analyst, Deyton began volunteering with a group of of LGBT health professionals to provide services to gay men from a church basement (Roeder, 2019). In 1978, he co-founded what is now Whitman-Walker Health as “a health clinic for gay men and lesbians before AIDS redefined everything and the clinic became a hub for HIV treatment” (Sullivan, 2011). Deyton eventually left his health policy analyst job to attend medical school at GW in 1981.
While in medical school, Deyton found a copy of Morbidity and Mortality Weekly Report (MMWR) dated June 5, 1981 that described cases of a “rare pneumonia among young, previously healthy gay men in Los Angeles” in his student mailbox (Roeder, 2019). While reading this report on what would eventually be known as HIV/AIDS, Deyton recalls “my heart sank. I knew something awful was happening to my community” (Roeder, 2019). HIV/AIDS became personal for Deyton. He still keeps a blue address book with the names of personal and professional contacts from this time. Roughly a third, about 50 people, in this contact book died (Roeder, 2019). “It’s a totem of remembrance and survival. I’ll never throw it out” Deyton says (Roeder, 2019).
While completing his residency at the University of Southern California Los Angeles County Medical Center, Deyton applied for a competitive position at the NIH. He almost didn’t make it to his interview due to a blizzard that slammed the East Coast the day before his interview. After catching the first available flight and renting a limo to drive him because no taxis were available due to the storm, Deyton arrived to an empty NIH building, “save for a building security guard and one man who didn’t believe in snowstorms shutting down the government” (GW SMHS, 2017). This is how his friendship with Dr. Anthony Fauci began.
As Dr. Fauci recalled during Deyton’s installation as the Murdock Head Professor of Medicine and Health Policy at SMHS, “the guard almost didn’t let him in, but he insisted, pleading with the guard - and this is a true story - he knew how compulsive I am and that I would be there and went up to the seventh floor, knocked on the door...I opened the door, and there began a 30-year relationship” (GW SMHS, 2017). Deyton got the NIH position. At the NIH, he played a crucial role in HIV/AIDS research during the early years of the 1990s epidemic, helping to lead more than 200 NIH-funded clinical trials on HIV therapeutics (Partnership for Public Service, 2021). He oversaw “clinical research on the development and approval of antiretroviral drugs and treatment strategies, including the first trials of combination therapies, the cornerstone of current HIV treatments” (GW SMHS, 2017).
During the course of this research, Deyton helped recruit thousands of HIV/AIDS patients into clinical trials that had “previously been excluded, such as African Americans, drug users, and those with little or no access to health care” (Partnership for Public Service, 2021). At a time when activists such as ACT UP were demanding to be active participants in HIV/AIDS research, Deyton developed the first NIH-funded community-based research program that “included front-line providers in places like LGBT health clinics, homeless shelters, and IV drug use programs'' (Roeder, 2019). “I cannot say how cutting-edge his approach was at the time,” said Margaret Hamburg, FDA Commissioner who nominated Deyton for a Samuel J. Heyman Service of America Medal (Deyton was a finalist for this prestigious award). “It brought research to communities that needed it. He understood the disconnect between patients and research, and he found a new way to do testing and develop products” (Partnership for Public Service, 2021).
By 1996, HIV/AIDS research had started to produce positive results. Deyton recalls being part of a Data and Safety Monitoring Board (DSMB) meeting in which the results of a double-blind NIH-funded study investigating if adding a third drug to suppress HIV would be more effective and extend survival. The unblinded results showed that the regimen was working! “It was one of the most powerful moments in my life. I remember sitting in the DSMB meeting and I started to cry, and I wasn’t the only one. People were living” (Roeder, 2019).
Deyton eventually left the NIH for a position at the US Department of Veterans Affairs as the director of HIV/AIDS treatment programs. At the time, the VA was the largest care provider for HIV-infected patients in the US (Sullivan, 2011). He became the Chief Public Health and Environmental Hazards Officer for the VA, overseeing all public health programs for the national VA health care system. Deyton then transitioned to the FDA, where he served as the first Director of the Center for Tobacco Products. In this role, he oversaw implementation and enforcement of the Family Smoking Prevention and Tobacco Control Act which, for the first time, gave FDA public health regulatory authority over tobacco products in the US.
Now, as the Senior Associate Dean for Clinical Public Health and the Murdock Head Professor of Medicine and Health Policy at GW SMHS, Deyton continues his legacy of creating positive change within healthcare. With SMHS’s strong commitment to social responsibility, it’s a great place for Deyton to do just that! In addition to his innovative Patients, Populations, and Systems course curriculum mentioned earlier, Deyton has been outspoken about influencing change in accrediting bodies within healthcare. Accrediting bodies “want to change...but they don’t know how” Deyton says in the video below.
“...I think the way we can help them do the right thing, is to learn from ACT UP, and learn from the gay rights movement, and learn from the women’s movement, and learn from the civil rights movement. Sometimes leaders just have to stand up, and take a stand, and march, and occupy... If we really believe [in] what we want to do, we have to stop wringing our hands, and take to the streets, and go tell our professional bodies what we need them to do.”
(UNM Health Sciences, 2015)
Deyton’s goal for the GW SMHS’ innovative Clinical Public Health curriculum and programs is to prepare GW students to not just be great clinicians at the bedside but also to recognize, speak up and act on those factors outside of the hospital and clinic that will improve their patients’ health. Deyton believes clinicians must use their experience and their voices to improve community health. A guiding theme in Deyton’s life, and one that he has shared with his students, has been to “Just speak. Say who you are and what you want to do, and don’t worry about what anybody else thinks” (Roeder, 2019). It’s no wonder that Deyton has been an inspiration to so many students and colleagues at SMHS!
George Washington University School of Medicine & Health Sciences. (2017, June 5). Murdock Head Professor of Medicine and Health Policy Installation [Image of Dr. Lawrence “Bopper” Deyton and Dr. Anthony Fauci]. [Photo Album]. GWSMHS Facebook page. https://www.facebook.com/pg/GWSMHS/photos/?tab=album&album_id=1458177520888127














{kind=link}