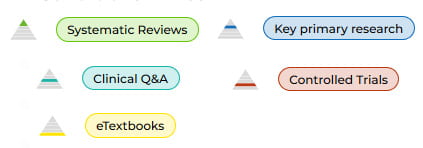
The Trip Database is a medical search engine with an emphasis on evidence based practice (EBP), clinical guidelines and queries. Himmelfarb Library provides access to the freely accessible version of Trip. Started in 1997, Trip aims to help users “find evidence fast” with an easy to use search interface that filters results based on the evidence pyramid. A pyramid icon is displayed with the resource that indicates where the resource falls on the evidence pyramid.
In addition to the journal articles, Trip results provide a full range of resources including e-textbooks, patient information leaflets, educational courses and news. One thing to keep in mind about Trip is that publishers are classified by their output. Cochrane is known for publishing systematic reviews, and therefore Cochrane published resources will appear in the Systematic Reviews filter. The New England Journal of Medicine (NEJM) is classified as Primary Research. This means that if a systematic review is published in NEJM, it will appear in the Primary Research filter. However, when a systematic review is reviewed by the Database of Abstracts of Reviews of Effects (DARE), it will eventually appear in the Systematic Reviews filter, although there is a time delay.
Trip can be used by practicing physicians who would like to broaden their background knowledge on conditions such as diabetes or cancer, or who need to find relevant evidence-based information on testing guidelines or to make sure a “don’t miss” diagnosis is included in their differential diagnosis. Trip is also useful for medical students who may find the PICO search tool an effective way to search for applicable resources. Check out this blog post to learn more about case studies for using Trip.
Trip has responded to the War in Ukraine by creating a combat injuries filter. While this effort is still a work in progress, the filter attempts to gather the best combat evidence available.
Interested in learning more about Trip? Check out the short video below:
In a 1955 Science article, Eugene Garfield proposed a citation index for the sciences (Garfield, 1955). The purpose was to make it easier to see which works cited or criticized a research paper, enabling researchers to find both frequently cited works and those that had flaws. The idea was that this would root out bad research and elevate that which had merit.
The first Science Citation Index was published in 1964. The indexes quickly became a staple tool for science and social science researchers, existing in print for decades and then going online and evolving into the present day Web of Science database. Researchers and faculty members in the sciences are now very cognizant of their h-index factor, a measure of the relevancy of their published works based on citation counts (this site explains how to calculate your h-index and the difference between Google Scholar’s and WOS indexes). Similarly the Journal Impact Factor emerged as a way to calculate the relevance of a scientific journal. Publishing in a high impact factor journal means more prestige for the author and the journal impact factor is a measure that librarians frequently use to make subscription decisions.
Some publishers and researchers have figured out ways to game the system over the years. Puffing up your h-index factor can win you grants and tenure. Similarly, inflating a journal’s impact factor means it will attract top researchers who want to publish their findings in it, as well as more subscriptions and revenue.
In 2013, Nature revealed a group of Brazilian journals had arranged to cite works from each other’s publications in a citation stacking scheme (Van Noorden, 2013). Journals have also found ways to manipulate impact factors by exploiting the types of content published. A recent analysis of the British Journal of Sports Medicine which had a sudden rise in impact factor found that there was a corresponding “exponential rise” in editorials published (Heathers, 2022). Publishing a large number of small citable items, like editorials, can boost impact factors due to the way they are calculated and this worked for BJSM, making it the top ranked sports medicine journal. Publishers also game the calendar by publishing items digitally and allowing them to accumulate citations before giving them an official publication date or “front loading” by publishing more research early in the year to accumulate additional citations when the impact factor calculation is run at the end of the year.
Richard Phelps at Retraction Watch recently wrote a brief article on citation cartels. Established scholars in a field cite each other’s works in an ‘I’ll scratch your back, you scratch mine’ type arrangement that is mutually beneficial. His analysis revealed how a group of ‘strategic scholars’ could boost their impact factors by three times over ‘sincere scholars’ over the course of a few years. This increases their influence and mutes the voices of others. It reinforces the old boys’ club aspect of scientific and medical research and is particularly problematic in light of diversity and equity concerns.
The fairness and effectiveness of impact factors has been addressed by the Declaration on Research Assessment (DORA). The declaration came out of the 2012 meeting of the American Society for Cell Biology in San Francisco. It is now an international initiative covering all scholarly disciplines. DORA confronts issues of consistency, transparency and equity in research assessment and calls for:
the need to eliminate the use of journal-based metrics, such as Journal Impact Factors, in funding, appointment, and promotion considerations;
the need to assess research on its own merits rather than on the basis of the journal in which the research is published; and
the need to capitalize on the opportunities provided by online publication (such as relaxing unnecessary limits on the number of words, figures, and references in articles, and exploring new indicators of significance and impact).
Garfield. (1955). Citation indexes for science; a new dimension in documentation through association of ideas. Science (American Association for the Advancement of Science), 122(3159), 108–111 https://www.science.org/doi/10.1126/science.122.3159.108
Heathers and Grimes. (2022). The Mechanics Behind A Precipitous Rise In Impact Factor: A Case Study From the British Journal of Sports Medicine. OSFPREPRINTShttps://osf.io/pt7cv/
3D printing – what is it? It is a method of production, also known as additive manufacturing, in which software guides a machine to craft a 3D object, often with a high level of detail. This, however, is a very generalized definition. It is easy to assume that there is only one kind of 3D printing, but on the contrary: there are many different types of 3D printing, which can be referred to as “processes.” This post seeks to elaborate upon the different 3D printing processes, from the traditional Fused Deposition Modeling that you can find here at Himmelfarb Health Sciences Library, to the more unusual powder bed 3D printing, which is often used in the production of metal objects.
If you difficultly visualizing any of these types of 3D printing processes while reading this piece, check out Horne & Hausman’s 3D Printing for Dummies Chapter 2: Exploring the Types of 3D Printing. This post will describe these processes using more current terms, but this chapter has clear diagrams and illustrations, as well as some additional information about how various 3D printing processes function.
The most popular process of 3D printing is Fused Deposition Modeling, often referred to as FDM printing. This process produces 3D objects by heating up long strings of plastic material (aka: spools of filament), fusing it to the base platform of the printer, then continuing to build it up layer by layer using that same fusion process. Another way of looking at FDM printing is that it’s akin to a highly-nuanced hot glue gun (Horne & Hausman, 2018). There are also variants of FDM printers that utilize pellets instead of filament spools (Volpato et al., 2015), as well as those that use a cold semi-liquid mixture like what you might see with large-scale 3D printed houses that use concrete extrusion (Borg Costanzi et al., 2018).
FDM printing has some limitations. When the filament is in a moldable state during FDM printing, it extrudes through a nozzle, which is almost always moved along X and Y axes like what you might see on a crane game. Because of those movement restrictions, this process is weaker compared to its alternatives when it comes to items that have overhangs or details on an object’s underbelly. The machine is not so sensitive to be able to tell the difference between the 3D printers’ base platform, the previously-placed layers, and open air, so the printer needs the guiding software to give the digital object file (which you can think of as a map or a layout) structures known as “supports” which are designed to be removable. When those supports are removed, it is not uncommon to see score marks on the places where it touched, and in some cases, the area is so narrow that it’s impossible to remove those supports (Horne & Hausman, 2018).
Supports are less of a concern with Stereolithography Apparatus 3D Printing, also known as SLA printing. This 3D printing process produces 3D objects by aiming a laser up into a vat of liquid photopolymerizing resin. Photopolymerizing means that the liquid will transform into a solid when light of a certain wavelength touches it. Unlike FDM printers, which move the entire nozzle horizontally, SLA printers keep the laser fixed in one place, but change the angle. As the software instructs the laser to solidify certain portions of the vat of resin, the object is raised up and out of the vat by a component called the “elevator.” In the case of SLA printers, supports are not needed in order to hold up layers that have overhangs, but instead to keep the object attached to the elevator. SLA printers allow for more complex structures with holes, divots, and overhangs without using up as much filament and without causing scoring marks, and they often manage to print simple objects faster than FDM printers (Horne & Hausman, 2018).
SLA printing has its own downsides to keep in mind. For one, SLA printers tend to be more expensive than FDMs, and they require extra equipment, such as curing stations. Once the object is lifted up and out of the vat, it exists in a semi-cured state and is sticky. It needs to be treated with UV light to finish it. This makes not only cost, but space a concern, particularly since there is liquid resin involved, which requires special storage and disposal methods (Horne & Hausman, 2018).
Powder bed printing, also known as binder jet printing, likewise has some advantages at the cost of specialized set-up requirements. During this 3D printing process, a printer head moves horizontally along X and Y axes like with FDM printing, dropping a liquid binding material onto a powder that covers the printers’ base platform. When the binder comes in contact with the powder, a chemical reaction occurs that solidifies it. Since this process requires the use of fine particles which could be made of metal, plastic, sand, or even plaster, powder bed printers often require hoods and filters to prevent users from breathing in potentially harmful materials. An alternative method of powder bed printing uses a laser in the place of the binding liquid, which burns the powder to solidify it, which adds to the amount of safety equipment required (Horne & Hausman, 2018).
The finished product requires a step known as “depowdering” which can be done by hand with brushes and through automated vibration. Manual depowdering with brushes takes a significant amount of time, whereas automated vibration tools tend to be rather expensive. If you want to learn more about depowdering, this webpage by German depowdering manufacturer Solukon could be of help (Solukon, n.d.).
Powder bed printing is incredibly fast compared to FDM and SLA printing, and it has the added benefit of being able to produce metal objects swiftly. Additionally, this method does not require the use of supports, since the underlying layers of powder that were not activated by the binding chemical or laser can still support the weight of the rest of the object, despite the fact that the head of this kind of printer generally stays on X and Y axes like FDM printers (Horne & Hausman, 2018).
We would be remiss to not mention bioprinting, a process that technically falls under the umbrella of 3D printing which produces natural tissue, often for the sake of testing medications. The process of bioprinting starts by packaging certain types of cells taken from a biopsy into pellets the size of a micrometer or within a liquid that keeps the cells alive. Next, these packaged cells are combined with nutrients and a support material known as a matrix; this combination is known as a bioink. This bioink is then put into place layer by layer by the printer which is guided by software that interprets CT scans and MRIs. Up to this point, bioprinting fits the description of 3D printing, though the materials used are beyond the norm (Wei et al., 2020).
This is where bioprinting diverges, though. Rather than cooling down or solidifying and going off to the post-processing clean-up stage, the cells consume the nutrients and grow within the matrix. Pressure and chemical stimuli are added very carefully to nudge the cells to grow in the intended ways, and chemicals known as bioreactors are added as well to increase the speed of cell growth. There is no kind of 3D printing that is like this, simply because this part of the bioprinting process is less reliant on 3D printing methods and more on natural process of life: consumption, reproduction, and maturation (Wei et al., 2020).
Additional niche 3D printing processes also exist. Laminated Object Manufacturing (LOM) is a process that builds up laser-cut layers of paper, metal foil, or plastic film that has been coated with chemicals of choice. This process uses cheap, readily available materials and allows for additional customization, as the material color can change between layers (Horne & Hausman, 2018). Unfortunately, non-industrial LOM printer manufacturers are few and far between, as they are outpaced in popularity by FDM and SLA printers.
RoboCasting, a method of 3D printing similar to FDM printing which uses a paste made up of materials such as glass or ceramic, which either hardens on its own or needs to be baked. In their work, “3D Printing Bioinspired Ceramic Composites”, Feilden et al. explain how RoboCasting functions and how it can be used to mimic natural materials such as bone and shell (Feilden et al., 2017). This has some benefits for medical sciences through the development of implants such as biodegradable bone scaffolds that can aid during the healing process of bones, which you can learn more about in this study by Lei et al. (Lei et al., 2020).
Each of these 3D printing processes has strengths and weaknesses. Some may be faster, others may be more precise, and others still may be cheaper. This variability makes some more suitable for certain applications than others. FDM, for instance, because of its popularity, limited cost, and low barrier to entry, makes it a perfect choice for early-stage prototyping, whereas powder-bed printing may be more suited for an industrial environment. With 3D printing, the sky is truly the limit, particularly since new printers are being developed each year.
Want to try out 3D printing yourself? We are proud to announce that we have moved to a free-to-print policy and will no longer be charging cost-recovery fees for most print jobs. Some limitations apply, so make sure to consult our 3D Printing at Himmelfarb guide or full policy for the full details.
Borg Costanzi, C., Ahmed, Z. Y., Schipper, H. R., Bos, F., Knaack, U., & Wolfs, R. J. H. (2018) 3D printing concrete on temporary surfaces: The design and fabrication of a concrete shell structure, Automation in construction, 94, p. 395-404 https://doi.org/10.1016/j.autcon.2018.06.013
Feilden, E., Ferraro, C., Zhang, Q., García-Tuñón, E., D'Elia, E., Giuliani, F., Vandeperre, L., & Saiz, E. (2017). 3D printing bioinspired ceramic composites, Scientific Reports, 7(1), p. 1-9. https://doi.org/10.1038/s41598-017-14236-9
Horne, R. & Hausman, K. K. (2018). Exploring the types of 3D printing. 3D Printing for Dummies. https://ebookcentral.proquest.com/lib/gwu/detail.action?docID=4856326
Lei, L., Wei, Y., Wang, Z., Han, J., Sun, J., Chen, Y., Yang, X., Wu, Y., Chen, L., & Gou, Z. (2020). Core–shell bioactive ceramic robocasting: Tuning component distribution beneficial for highly efficient alveolar bone regeneration and repair, ACS biomaterials science & engineering, 6(4), p. 2376-2387. https://doi.org/10.1021/acsbiomaterials.0c00152
Solukon. (n.d.). Automating depowdering in 3D printing. Retrieved May 8. 2022 https://www.solukon.de/en/news/festo-and-solukon/
Volpato, N., Kretschek, D., Foggiatto, J. A., & Gomez da Silva Cruz, C. M. (2015) Experimental analysis of an extrusion system for additive manufacturing based on polymer pellets, International journal of advanced manufacturing technology, 81(9-12), p. 1519-1531. https://doi.org/10.1007/s00170-015-7300-2
Wei, S., Starly, B., Daly, A. C., Burdick, J. A., Groll, J., Skeldon, G., Shu, W., Sakai, Y., Shinohara, M., Nishikawa, M., Jang, J., Cho, D., Nie, M., Takeuchi, S., Ostrovidov, S., Khademhosseini, A., Kamm, R. D., Mironov, V., Moroni, L., Ozbolat, I. T. (2020). The bioprinting roadmap. Biofabrication, 12(2). https://doi.org/10.1088/1758-5090/ab5158
Saturday, May 21, 2022 is recognized as World Day for Cultural Diversity for Dialogue and Development. This awareness day was first established by the United Nations in 2002 and is a day that recognizes the importance of cultural diversity as a way to overcome long-standing divisions, cultivate global peace and sustainable economic growth.
“Three-quarters of the world’s major conflicts have a cultural dimension. Bridging the gap between culture is urgent and necessary for peace, stability and development. Cultural diversity is a driving force of development, not only with respect to economic growth, but also as a means of leading a more fulfilling intellectual, emotional, moral and spiritual life.” (United Nations, n.d.)
If you’d like to honor World Day for Cultural Diversity for Dialogue and Development, here are some resources, organizations and events that can assist you:
Passport DC- Organized by Cultural Tourism DC, Passport DC occurs in May and is a month-long event filled with concerts, festivals, panel discussions and much more that highlights the rich culture of different countries and ethic groups. The Around the World Embassy Tour is likely Passport DC’s most well-known event, where many embassies open their doors to the general public and showcase their country’s cuisine, art, music or other cultural staple. 2022’s Around the World Embassy Tour occurred earlier this month, but Passport DC has a plethora of upcoming events including ‘Matcha Teabowls special exhibition at TOKIYA’, ‘The Washington Jewish Film and Music Festival’, ‘Argentine Festival’, and ‘Taiwan Night Concert 2022’. Visit Passport DC’s website to learn more.
GW’s Office of Diversity, Equity and Community Engagement- GW’s Office of Diversity, Equity and Community Engagement offers events, educational resources and much more in an effort to establish an inclusive atmosphere and encourage productive dialogue about diversity, equity and inclusion on campus. Currently, they are disseminating a Spring 2022 Climate Survey to “gather information about the current university climate related to diversity, equity, and inclusion for students, faculty, and staff.” (Office of Diversity, Equity and Community Engagement, n.d.) May 20th is the last day to submit the survey. The office also offers resources on allyship, decolonization, gender and sexuality and so much more.
Himmelfarb’s Cultural Competency Guide- This guide provides educational materials to help researchers and students navigate cultural awareness in the medical and health sciences field. The guide has several tabs for specific resources such as books, articles, clinical resources and more. This is a living guide with new resources added as they are made available. If you have questions or would like to offer additional resources, please contact Stacy Brody at sbrody98@gwu.edu.
By interacting with different cultures we not only better understand ourselves, but we also connect with others on a deeper and meaningful level. World Day for Cultural Diversity for Dialogue and Development is the perfect opportunity to engage with a worldview that’s outside of your own!
You may have already heard, May is Mental Health Awareness Month. In order to cultivate a better understanding and to educate theGW community, GW is hosting interviews with a panel of experts available throughout the month of May. These professionals are well equipped to answer questions on various topics that may relate to marginalized populations, teacher/student, adolescent and youth health, war and conflict, and more. If you are interested in scheduling an interview with one of GW’s experts, please contact GW Media relations at gwmedia@gwu.edu.
It is also critical to understand that your mental health matters, and GW cares. If you feel like you are overwhelmed or stressed, GW offers Counseling & Psychological services that are confidential and safe for our students, staff and faculty members. No appointment is necessary; walk-ins are welcome.
The GW Office of Integrative Medicine and Health offers a number of resources to GW employees through its GW Resiliency and Well Being Center. Contact them to schedule educational talks, group workshops, or individual coaching on a number of topics including stress management, substance abuse, self-care and lifestyle (mindful eating, restorative sleep, etc.). And check out theOffice of Integrative Medicine and Health’s weekly A Mindfulness Experience online sessions on Fridays from 2-3 pm addressing online stress relief, immune system support, and evidence based answers to COVID-19 questions. The sessions include a 30 minute mind-body practice.
Just as our physical health is vital to a healthy life, so is our mental health. Remember, GW is here for you.
Spring is a time of renewal and growth following the cold winter months, and it's also time to renew (or newly set up) your Lexicomp app!
Lexicomp is a comprehensive clinical drug information app including Lexi-Drugs, a drug interaction tool, and an extensive library of clinical calculators. Lexicomp is available both via web access and as an app that you can install on your phone (iPhone or Android), iPad, or other handheld device.
The Lexicomp app is free and Himmelfarb Library’s subscription allows you to install Lexicomp‘s high-quality drug information to your phone, iPad, or other handheld device. Follow the below instructions to obtain Lexicomp app access at no charge via Himmelfarb Library's license!
Lexicomp app renewals:
Access Lexicomp then click on Mobile Access Codes; select your platform (iOS or Android) and Returning Customer, then copy the displayed Authorization Code.
In the Add a Subscription by Code section, paste the authorization code.
You will receive an email with a 5-character PIN at your registered email address; enter the PIN into the Verify PIN field then click Verify.
Click Finish
On your phone/iPad/handheld, open the Lexicomp app and update.
New Lexicomp app users:
Access Lexicomp, then click on Mobile Access Codes; select your platform (iOS or Android) and New Customer, then copy the displayed Authorization Code.
This weekend marks GWU’s 2022 Commencement! From Thursday through Sunday, the campus will be filled with graduates dressed in their regalia, family and friends snapping pictures, and students, staff and faculty members applauding the accomplishments and hard work of their peers.
The staff at Himmelfarb Library would like to take this opportunity to recognize all of the graduates in the School of Nursing, Milken Institute School of Public Health and the School of Medicine and Health Sciences. We’ve thoroughly enjoyed working with you both in and out of the classroom, addressing your information needs and helping you navigate your academic and research interests. We know you will continue to achieve your goals as you transition into your career or continue to navigate academia and scholarly publishing. Once the dust settles on graduation, be sure to check out GW’s E-Resources for Alumni!
Here are some resources and brief reminders for Sunday’s Commencement ceremony. The event will begin at 10:30 am on the National Mall. Graduates should arrive by 8:30 am and line up with their school. Please wear your graduation regalia and bring your Commencement credential with you. GWU’s Commencement Details page provides more information such as the ceremony’s COVID-19 safety measures, a graduate checklist, a list of prohibited items and a detailed schedule. If you’re posting pictures from the ceremony on your social media accounts, be sure to tag us on Twitter, Instagram, or Facebook so we can celebrate with you!
Congratulations Class of 2022! Though we’ll miss seeing you on campus and in Himmelfarb, we know you will continue to make us proud and we are eager to see what accomplishments and accolades await you in the future!
Did you know himmelfarb has a bookshelf on the 1st floor that is reserved for you?
We call it the “take a book, leave a book” bookshelf, and it works exactly the way it sounds. The take a book, leave a book shelf is in the nook area next to the Humanities and Health Collection. If you’re familiar with little free libraries, this is the same concept. We invite you to take any of the books on the shelf for personal reading. There is no need to check them out at the circulation desk.
Do you have books at home that are collecting dust, or do you have a few titles that you would like to share with your classmates? Feel free to leave them on the “take a book, leave a book” shelf. Keep in mind that leaving a book is discarding the book - these titles are not added to our collection, and we do not keep track of them. That being said, isn’t it fun to try something new? Who knows, you might find your next favorite book on our take a book, leave a book bookshelf!
In an effort to remain accountable to communities who have been negatively impacted by past and present medical injustices, the staff at Himmelfarb Library is committed to the work of maintaining an anti-discriminatory practice. We will uplift and highlight diverse stories throughout the year and not shy away from difficult conversations necessary for health sciences education. To help fulfill this mission, today’s blog post will highlight data disaggregation and how it can address health disparities within the Asian-American, Native Hawaiin and Pacific Islander communities.
As health researchers and medical professionals, data collection and management is necessary for discovering emerging health trends and understanding how behavioral changes can impact a patient's quality of life. But the way data is collected and interpreted can generate misleading information for certain communities.
When filling out surveys or federal documents, for example new patient intake forms, job applications, or the U.S. Census survey, there’s a section that asks for race and ethnicity. There are typically a minimum of five selections for race : American Indian or Alaska Native, Black or African American, Asian, Native Hawaiian or Other Pacific Islands, and White. These categories are the minimum requirement as established by the Office of Management and Budget’s (OMB) 1997 ‘Revisions to the Standards for Classification of Federal Data on Race and Ethnicity.’ According to the standards, “Data were needed to monitor equal access in housing, education, employment, and other areas, for populations that historically had experienced discrimination and differential treatment because of their race or ethnicity. The standards are used not only in the decennial census…but also in household surveys, on administrative forms (e.g., school registration and mortgage lending applications), and in medical and other research.” (Office of Management and Budget (OMB), 1997, p. 58782) Within health sciences research, these racial categories allow researchers to understand health concerns within specific communities and can lead to preventative health measures that are tailored to a community’s concerns. But many researchers are pushing for data disaggregation which can highlight disparities that are otherwise overlooked when using broad racial categories such as ‘Asian’ or ‘Pacific Islander.’
“Asia consists of over forty countries, and the Pacific Islands are grouped by three subregions of Oceania (including Native Hawaiians); both have a diaspora spread across the globe. Due to differences in social, economic, and environmental factors, it is erroneous to assume that health disparities for this population do not exist.” (Bhakta, 2022, p. 133)
Adia et. al examined the results of a California Health Interview Survey (CHIS) conducted from 2011-2017 and found that while the aggregated data suggested Asian Americans in the state appeared healthier than non-Hispanic Whites, when the data was broken into specific subgroups that fall under the Asian category many health disparities, such as high blood pressure, diabetes or asthma, were uncovered. For example, when examining the rates of high blood pressure among survey responders, 31.0% of Non-Hispanic White respondents reported having high blood pressure compared to 22.9% of All Asian respondents. But when examining specific subgroups, the researchers found that 32.3% of Filipino and Japanese respondents reported having high blood pressure. (Adia et al., 2020) “Overall, these findings support further data disaggregation in other large-scale research efforts to support interventions tailored specifically to Asian subpopulations in need…Disaggregation showed that each Asian subgroup faced disparities in health condition, outcomes, and service access that would have been masked.” (Adia et al., 2020, p. 525) When health data is disaggregated, researchers may be alert to concerning medical trends in specific communities and can work with local community partners to implement preventative screenings or devise treatment plans that allow patients to receive the best care possible. Adia et al. also noted that their findings are not applicable to Asian and Pacific Islander populations in other parts of the United States as the makeup of these populations will differ from state to state, which further highlights the need to conduct research in other communities across the country.
In order to gather accurate data and combat health inequities within the Asian American and Pacific Islander communities, researchers will need to partner with local community members and find solutions that prevent people from accessing proper care. In a 2020 article for Cronkite News, Laura Makaroff, Senior Vice President for Prevention and Early Detection at the American Cancer Society, said, “To make a big difference and seriously impact and reduce health inequities in Asian American populations…we need to address language access, be culturally competent, really support and engage partnerships and collaborations, include communities and people in all of research, and really be responsive and accountable to all of the different Asian American communities we serve…We need to begin and end with the community.”(Gu, 2020) Like other communities of color in the country, some sections of the Asian American and Pacific Islander communities do not fully trust the medical community. To bridge that divide, researchers will need to partner with local leaders and trusted institutions, such as religious centers, community centers, public libraries or cultural organizations, who are embedded in these communities and have a deep understanding of community members’ concerns. There are numerous ways to conduct medical research that is accessible and the local leaders and institutions can provide valuable insight to researchers.
To learn more about data disaggregation as it relates to the Asian American and Pacific Islander communities, please read any of the works cited in this article or listed in the reference section below. The importance of data disaggregation is an ongoing conversation and we hope this article will encourage you to think critically about this topic and share your ideas and solutions with your colleagues.
Yi, S.S. (2020). Taking Action to Improve Asian American Health. American Journal of Public Health(1971), 110(4), 435–437. https://doi.org/10.2105/AJPH.2020.305596
Le, Cha, L., Han, H.-R., & Tseng, W. (2020). Anti-Asian Xenophobia and Asian American COVID-19 Disparities. American Journal of Public Health (1971), 110(9), 1371–1373. https://doi.org/10.2105/AJPH.2020.305846
Adia, Nazareno, J., Operario, D., & Ponce, N. A. (2020). Health Conditions, Outcomes, and Service Access Among Filipino, Vietnamese, Chinese, Japanese, and Korean Adults in California, 2011-2017. American Journal of Public Health (1971), 110(4), 520–526. https://doi.org/10.2105/AJPH.2019.305523
Bhakta, S. (2022). Data disaggregation: the case of Asian and Pacific Islander data and the role of health sciences librarians. Journal of the Medical Library Association, 110(1), 133–138. https://doi.org/10.5195/jmla.2022.1372
Panapasa, Jackson, J., Caldwell, C. H., Heeringa, S., McNally, J. W., Williams, D. R., Coral, D., Taumoepeau, L., Young, L., Young, S., & Fa’asisila, S. (2012). Community-Based Participatory Research Approach to Evidence-Based Research: Lessons From the Pacific Islander American Health Study. Progress in Community Health Partnerships, 6(1), 53–58. https://doi.org/10.1353/cpr.2012.0013
Executive Office of the President, Office of Management and Budget (OMB), Office of Information and Regulatory Affairs. (1997). Revisions to the Standards for the Classification of Federal Data on Race and Ethnicity. https://www.govinfo.gov/content/pkg/FR-1997-10-30/pdf/97-28653.pdf
Bates’ Guide to Physical Examination and History Taking is the premier textbook for instruction on physical exam, patient history taking, and assessment concepts and is currently in its 13th edition. Himmelfarb also subscribes to the audiovisual complement to Bates which includes substantial video content on physical examination, OSCE clinical skills, communication and interpersonal skills. Videos demonstrate head to toe exams and systems based exams.
Screenshot from Bates Visual Guide to Physical Examination
Over twenty new videos recently became available which provide training on communication skills and working with specific patient populations!
Technique: Active or Attentive Listening (1:47)
Technique: Guided Questioning (5:20)
Technique: Empathic Responses (3:31)
Technique: Summarization (2:03)
Technique: Transitions (2:03)
Technique: Empowering the Patient (3:14)
Technique: Reassurance (1:53)
Use of Understandable Language (3:41)
Use of Non-Stigmatizing Language (1:57)
Appropriate Nonverbal Communication (3:37)
Use of Preferred Title, Name, and Gender Pronoun (3:42)
Interprofessional Communication (3:12)
Patient-Centeredness in Computerized Clinical Settings (4:45)
Teach-Back Method (4:06)
Rapport: Newborns and Infants (1:58)
Rapport: Young Children (2:08)
Rapport: Adolescents (2:55)
Rapport: Older Adults (2:48)
Rapport: Patients with Physical and Sensory Disabilities (5:50)