
Resident Author: Jennifer Rabjohns
Faculty Mentor: Massoud Kazzi
Date of Presentation: 1/24/2019
Introduction:
40yoM, h/o EtOH abuse, found unresponsive at home.
EKG is below (@ 1030):
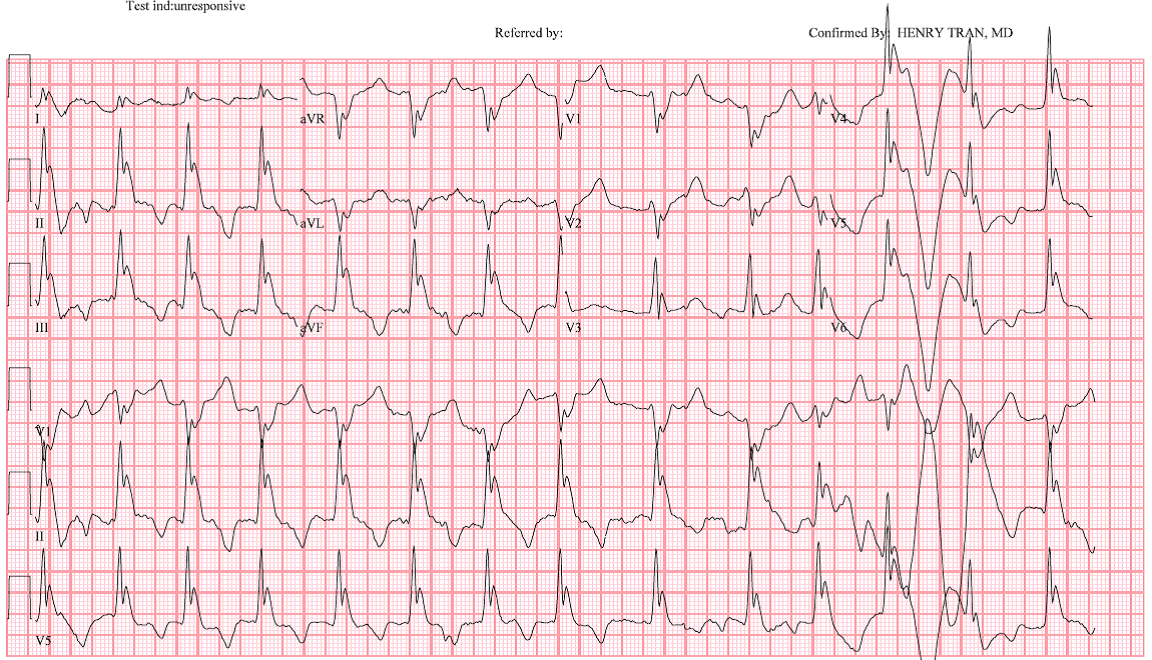
How would you describe this EKG?
Rate is about 80. It's hard to see P waves, but they're there, and they're all different; rhythm is irregularly irregular (atrial fibrillation). EKG machine reads a LBBB (however, does not meet LBBB criteria because aVL is down). QRS has an extra notch at the end. Deep inferolateral T wave inversions.
What is the differential diagnosis?
This extra notch at the end of the QRS is right before the J point. See examples here from LITFL:
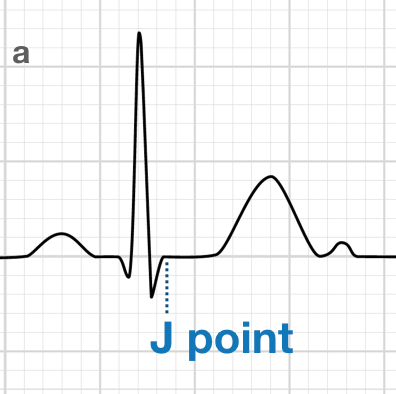

(For a review of J points, see the last blog post.)
From this review article, J waves (also known as Osborn waves) are associated with hypothermia but can also be seen in vasospastic angina, idiopathic ventricular fibrillation, cardiopulmonary arrest from oversedation, hypercalcemia, brain injury, and subarachnoid hemorrhage.
According to Dr. Smith's ECG Blog, the differential includes the above plus Brugada syndrome and benign early repolarization.
From Tintinalli's, J waves usually are seen at temperatures <32C.
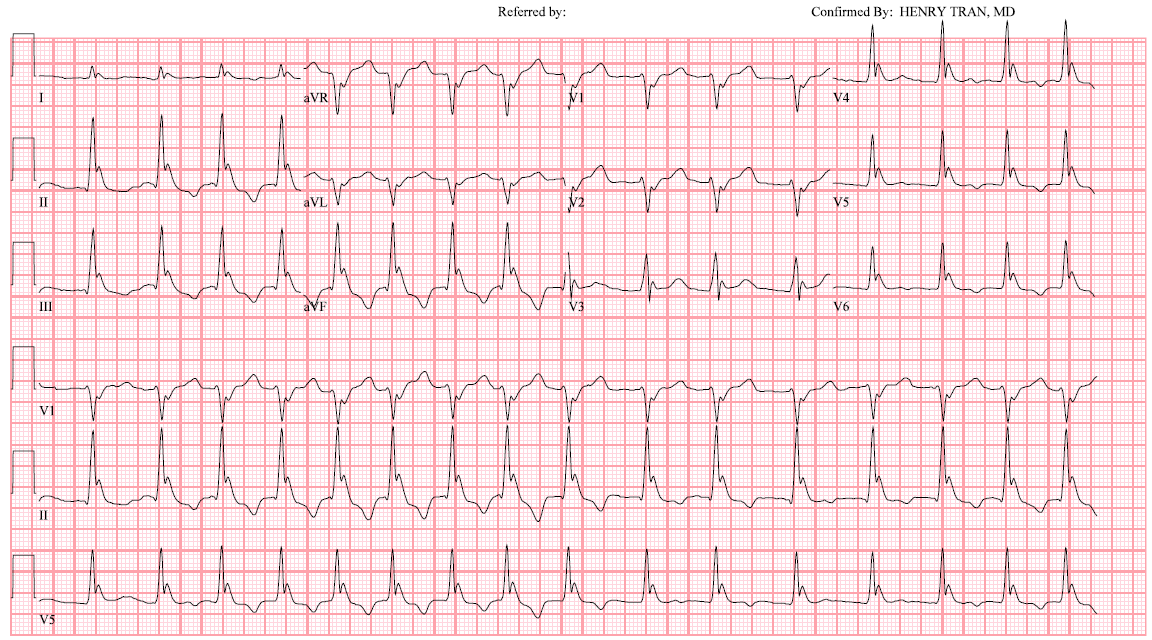
For this patient, we don't have an initial core temperature. For his second EKG (@ 1045), his core temperature was 28C (82F). The Osborn waves are smaller, which is to be expected as patients become warmer.
Second EKG (@ 1045):
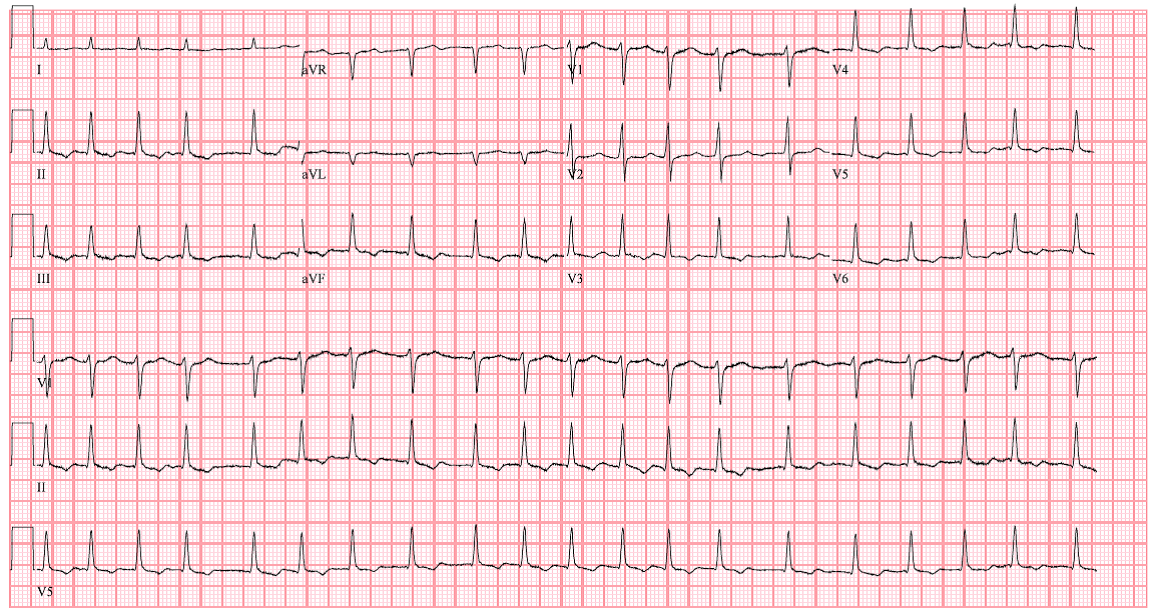
The patient was still being rewarmed during his third EKG (@1530, as inpatient):

Patient was normothermic for his fourth EKG (@ 430am the next day):
Tintinalli's notes that atrial fibrillation and flutter are expected. Other things you should know about hypothermia and EKG's - hypothermic J waves also have an arrhythmogenic potential that is proportional to the size of the J wave and not fully understood. Hypothermia can also cause any type of heart block or atrial/ventricular arrhythmias; be careful handling patient to minimize triggering them!
Take-home points:
- Use your history and physical if you see J waves, since the differential diagnosis includes hypothermia and other processes.
- J (Osborn) waves are usually seen at <32; as you warm your patients, their amplitude should go down.
- Be careful moving your hypothermic patients; rough handling can trigger arrhythmias.
References:
- Links as above.
- Brown D. Hypothermia. In: Tintinalli JE, Stapczynski J, Ma O, Yealy DM, Meckler GD, Cline DM. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8eNew York, NY: McGraw-Hill; 2016. http://accessmedicine.mhmedical.com/content.aspx?bookid=1658§ionid=109385768. Accessed January 26, 2019.