
EKG Contributor: Allen Wang, MD
Resident Author: Jennifer Rabjohns, MD
Faculty Mentor: Massoud Kazzi, MD
Date of Presentation: 5/24/19
Introduction:
40yoF presents after taking extra verapamil 2 hours ago. Her systolic blood pressure is persistently in the 70s but she's mentating well.
EKG:

How would you describe this EKG?
Rate is about 75 and normal sinus. Normal axis. First degree AVB. Borderline long QT.
What is the differential diagnosis?
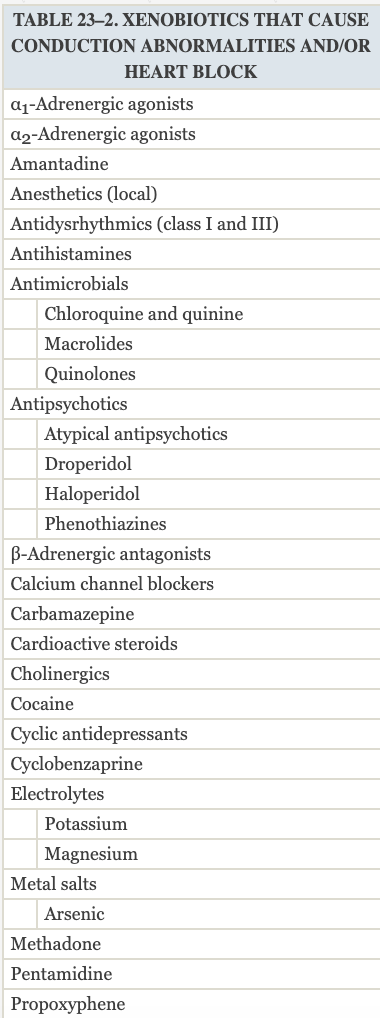
Goldfrank's has an extensive list of medications that can cause conduction abnormalities, included here because there are some medications that are surprising (1).
But back to the more common scenario - calcium channel blocker vs beta-blocker overdose. Goldfrank's notes it is very hard to distinguish based on EKG. But they note a few principles:

Beyond EKG's and looking more generally at the patient, Goldfrank's notes:
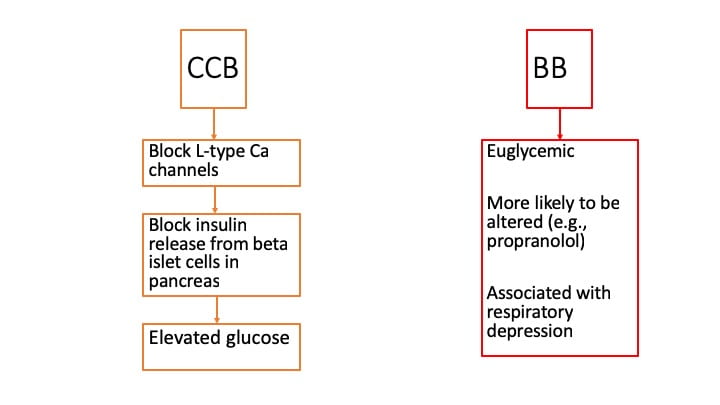
For this patient, her glucose was 140.
Background:
As alluded to above, verapamil and diltiazem (non-dihydropyridines) are associated with more myocardial effects.
Regular release formulations of calcium channel blockers have onset of signs and symptoms at 2-3 hours post-ingestion. Patients who take sustained release formations usually have onset of symptoms at 6-8 hours (1).
Management:
Goldfrank's has specific recommendations.
- Continuous cardiac monitoring
- EKG q1-2 hours
- Fluid bolus PRN hypotension
- Because of the significant danger of calcium channel blocker overdose, strongly consider orogastric lavage; recognize patients may have vagal response to it (worsening bradycardia and hypotension)
- Activated charcoal
- Whole bowel irrigation, especially if sustained-release ingestion
Pharmacologically, evidence for efficacy is lacking but you can try to work around the calcium channel blockage. Goldfrank's recommends the following sequence:
- Atropine (ACLS dosing); anticipate treatment failure
- Calcium: 10–20 mL of 10% calcium chloride or 30–60 mL of 10% calcium gluconate), repeat q15–20 minutes up to 3–4 doses or start continuous infusion
- Catecholamine such as norepinephrine,
- High-dose insulin infusion: if glucose is <250 mg/dL, give 25–50 g of dextrose (0.5–1 g/kg) followed by a dextrose infusion of 0.25–0.5 g/kg/h. Then give insulin bolus of 0.1 U/kg, followed by an insulin infusion (0.5 U/kg/h).
- Glucagon, 3-5mg given over 1-2 minutes
- Phosphodiesterase inhibitor (e.g., milrinone), using standard CHF dosing
Take-home points for calcium channel overdose:
- ABC's first
- Early decontamination is critical
- Serial EKG's (q1-2h)
- Pharmacologic sequence is atropine, calcium, catecholamine, high dose insulin/glucose, glucagon, and phosphodiesterase inhibitor
References:
-
Flomenbaum, N. & Goldfrank, L. & Hoffman, R. & Howland, M. & Lewin, N. & Nelson, L. (2006). ELECTROCARDIOGRAM DISTURBANCES. Goldfrank's Toxicologic Emergencies. Retrieved May 24, 2019 from https://www.r2library.com/Resource/Title/0071437630/ch0005s0085