
May 18, 2017
Emergency care for sepsis has evolved considerably over the past two decades. Prior to the Rivers trial in 2001, antibiotics were the mainstay of treatment, which then evolved into early resuscitation with intravenous fluids, blood products, invasive monitoring, and vasopressors.(1) In the past year, results from the Process, Promise, & Arise trials, then their recent PRISM meta-analysis challenged the concept of the important of invasive monitoring, but still underscore the benefits of early antibiotics and aggressive resuscitation (2,3,4,5).
Through this process and evolution, there has been a dramatic reduction in sepsis related mortality. Current approaches to sepsis resuscitation focus on the host by reducing hypo-perfusion. However, few effective therapies focus on the host response.Efforts to impact the host response have been disappointing after initial success, specifically with using steroids and activated protein C to treat sepsis (6,7, 8,9,10).
In recent months there has been a new development in sepsis, specifically a recent study by Paul Marik, published in CHEST. (11) Marik’s study tests a "sepsis cocktail", consisting of vitamins C & B1, combined with steroids, along with standard treatments for sepsis. In the trial, each of the components of his cocktail has been tested individually before, and showed some promise. For example, burn patients who receive Vitamin C require less fluids & produced more urine (12). Similarly, surgical ICU patients who were given Vitamin C had less ventilator days & less multiorgan failure (13). Patients with severe sepsis who were given Vitamin C had better SOFA scores (14), reduced mortality, & reduced vasopressin use (15). Thiamine too, has been shown to reduce mortality in septic shock among patients with thiamine deficiency (16). The addition of steroids in Marik's study was probably because of its synergistic effects with vitamin C (17).

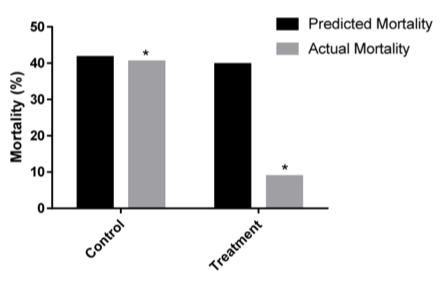
In the Figures, we see quite dramatic results with a great reduction in mortality in treatment as compared to the control arm, albeit this was a before-after study with historical controls. In addition, we see a significant reduction in SOFA scores – a measure of severity of illness. But before we say "Eureka", we need to carefully consider how to interpret these results. In the past, we have been tricked before by single center studies (even Randomized Controlled Trials), not to mention this was a before-after trial. Furthermore, it is unclear what the hidden harms may be (we've been fooled before by the benign nature of steroids & tight glycemic control in sepsis, only to find harms in external validation trials(6,7, 8)).
Are we going to face yet another disappointment once others try to replicate these results, or are we on the brink of a new sepsis break-through? We're a few rigorous trials short of getting that answer.
References:
- Early Goal-Directed Therapy in the Treatment of Severe Sepsis and Septic Shock. N Engl J Med 2001; 345:1368-1377
- A Randomized Trial of Protocol-Based Care for Early Septic Shock. The ProCESS Investigators*. N Engl J Med 2014; 370:1683-1693
- Trial of Early, Goal-Directed Resuscitation for Septic Shock. the ProMISe Trial Investigators. N Engl J Med 2015; 372:1301-1311
- Goal-Directed Resuscitation for Patients with Early Septic Shock. The ARISE Investigators and the ANZICS Clinical Trials Group. N Engl J Med 2014; 371:1496-1506
- Early, Goal-Directed Therapy for Septic Shock — A Patient-Level Meta-Analysis. The PRISM Investigators*. March 21, 2017DOI: 10.1056/NEJMoa1701380
- Effect of Treatment With Low Doses of Hydrocortisone and Fludrocortisone on Mortality in Patients With Septic Shock. JAMA. 2002;288(7):862-871
- Hydrocortisone Therapy for Patients with Septic Shock. the CORTICUS Study Group. N Engl J Med 2008; 358:111-124
- Effect of Hydrocortisone on Development of Shock Among Patients With Severe Sepsis: The HYPRESS Randomized Clinical Trial. JAMA. 2016 Nov 1;316(17):1775-1785
- Efficacy and Safety of Recombinant Human Activated Protein C for Severe Sepsis. the Recombinant Human Activated Protein C Worldwide Evaluation in Severe Sepsis (PROWESS) Study Group. N Engl J Med 2001; 344:699-709
- Drotrecogin Alfa (Activated) in Adults with Septic Shock. the PROWESS-SHOCK Study Group. N Engl J Med 2012; 366:2055-2064
- Marik PE et al. Hydrocortisone, Vitamin C and Thiamine for the Treatment of Severe Sepsis and Septic Shock: A retrospective Before-After Study. Chest 2016. S0012-3692(16)62564 – 3.
- Reduction of resuscitation fluid volumes in severely burned patients using ascorbic acid administration: a randomized, prospective study. Arch Surg. 2000 Mar;135(3):326-31.
- Randomized, prospective trial of antioxidant supplementation in critically ill surgical patients. Ann Surg. 2002 Dec;236(6):814-22
- Phase I safety trial of intravenous ascorbic acid in patients with severe sepsis. Journal of Translational Medicine, 2014, 12:32
- Effect of high-dose Ascorbic acid on vasopressor's requirement in septic shock. J Res Pharm Pract. 2016 Apr-Jun;5(2):94-100
- Randomized, Double-Blind, Placebo-Controlled Trial of Thiamine as a Metabolic Resuscitator in Septic Shock: A Pilot Study. Crit Care Med. 2016 Feb;44(2):360-7
- "Vitamin S" (Steroids) and Vitamin C for the Treatment of Severe Sepsis and Septic Shock! Crit Care Med. 2016 Jun;44(6):1228-9