

A patient presents to the emergency department presenting with precordial chest discomfort, pain radiating to the jaw, dyspnea, and diaphoresis. These are some of the typical symptoms highly indicative of acute coronary syndrome (ACS) [i]. However, not all patients have “typical” symptoms. Prior studies have shown that certain demographic groups, specifically patients of older age, black or Asian race, and female gender are less likely to present with these typical symptoms despite later having the diagnosis of ACS [ii]. In addition, other factors have been associated with atypical presentations including older age, and the presence of comorbid conditions such as diabetes.
While there is a large literature on atypical presentations of ACS, the combination of demographic factors – specifically combinations of race and gender – has not been closely explored until now. A recent study by researchers Drs. Ahmed Allabban, Judd Hollander and Jesse Pines at the George Washington University School of Medicine and Thomas Jefferson University published in the Emergency Medicine Journal focused on the combination of race and gender, and how the intersection of these two factors correlate with presentation of 30-day ACS or other serious cardiopulmonary diagnoses [iii]. The four subgroups were analyzed: black males, white males, black females, and white females.
The study was a secondary analysis of data collected from a prospective, observational cohort study of ED patients presenting with chest pain, with timeframe spanning from 1999 to 2008. The entire dataset was more than 4000 patients, and the study was conducted at an inner city academic hospital. Inclusion criteria included 30 years of age or older, presentation of chest pain where an ECG was ordered, and provision of informed consent. Patients who had chest trauma within the past week, a measured temperature of 101°F, used home oxygen, had metastatic cancer or had symptoms of palpitation alone without chest pain were excluded from the study.
The study found that symptoms associated with a higher risk of ACS in white males were left arm radiation, chest pressure and tightness, and substernal chest pain. These are typical symptoms of ACS. For black males, the symptom associated with a higher risk of ACS was diaphoresis. For black females, symptoms indicating higher risk of ACS included diaphoresis, palpitations, and left arm radiation, while symptoms indicating lower risk for ACS included pleuritic chest pain and left anterior chest pain. No symptoms were predictive of ACS for white females. For serious cardiopulmonary diagnoses, there were largely similar findings. Results are displayed in the figure below.
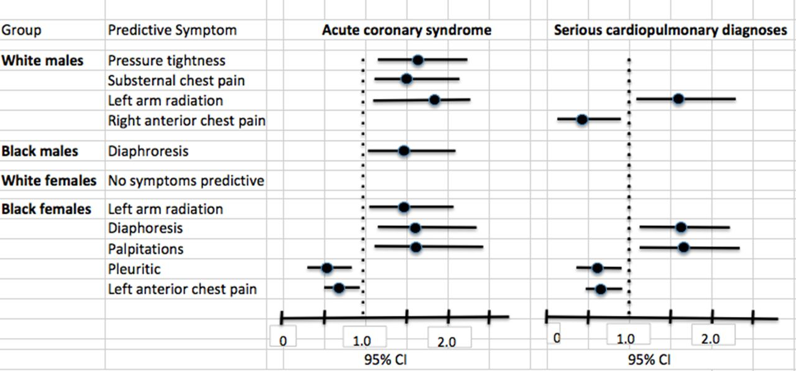
The data demonstrates that dividing patient populations by a combination of race and gender produces variably predictive symptoms of both ACS and other serious cardiopulmonary diagnoses. Thus, relying on a particular set of typical symptoms regardless of demographic representation may not be an optimal form of practice.
This study had several limitations, including being a single center study, using convenience sampling, and having variations in sample size for each subgroup. Further, while this study highlights differences in symptoms among race and gender subgroups, the question of what causes these differences remains an area to be explored. Preliminary explanations include hormonal, physiological, and sociocultural differences among each of these subgroups, though these have not been substantiated. The main takeaway is that physicians in the ED should keep these symptomatic differences between race and gender in mind when assessing a patient for chest pain.
[i] Ayman El-Menyar et al., “Atypical Presentation of Acute Coronary Syndrome: A Significant Independent Predictor of in-Hospital Mortality,” Journal of Cardiology 57, no. 2 (March 2011): 165–71, doi:10.1016/j.jjcc.2010.11.008.
[ii] H. Lee et al., “Typical and Atypical Symptoms of Myocardial Infarction among African-Americans, Whites, and Koreans,” Critical Care Nursing Clinics of North America 13, no. 4 (December 2001): 531–39.
[iii] Ahmed Allabban, Judd E. Hollander, and Jesse M. Pines, “Gender, Race and the Presentation of Acute Coronary Syndrome and Serious Cardiopulmonary Diagnoses in ED Patients with Chest Pain,” Emerg Med J, June 16, 2017, emermed-2016-206104, doi:10.1136/emermed-2016-206104.
Austin Wu is a medical student at the GW School of Medicine & Health Sciences
.jpg)

.png)