
Greg Jasani
August 2, 2017
Febrile neutropenia is a well known side effect of chemotherapy and patients with it often present to emergency departments. Standard of care has been to admit these patients for aggressive IV antibiotics. However, recent research has suggested that a certain subset of these patients can be considered low risk and managed as outpatients[1],[2]. Two risk stratification tools, the Multinational Association for Supportive Care in Cancer (MASCC) and Clinical Index of Stable Febrile Neutropenia (CISNE) scores, have been proposed to identify these low risk patients[3]. While these scores have been studied and validated in the inpatient setting, there has been no research about whether these risk stratification tools are valid in the emergency department. A recent article in Annals of Emergency Medicine by Coyne et al examined whether these scores could be used to accurately identify low-risk febrile neutropenic patients in the emergency department.
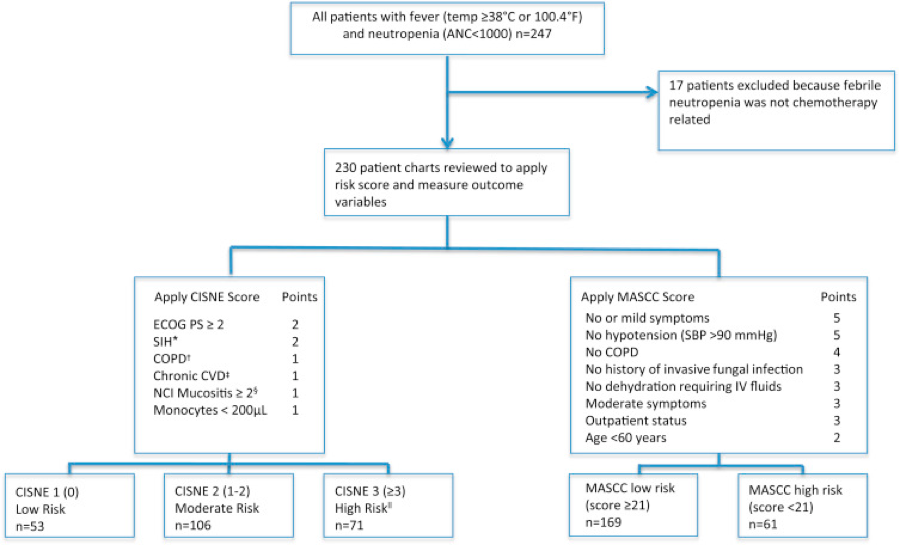
The study was a retrospective cohort study conducted in the emergency departments of two academic hospitals. It examined the medical records of all patients who presented with febrile neutropenia to the two emergency departments between June 2012 and January 2015. Inclusion criteria for the study were a fever of greater than 100.4F and an absolute neutrophil count of less than 1,000. Only patients with febrile neutropenia believed to be secondary to chemotherapy were included. In total, the authors reviewed 230 charts in their final analysis. The primary outcomes of the study were inpatient length of stay, level of care, clinical deterioration, clinical deterioration, positive blood cultures, and death. For the purposes of the study, the authors considered patients who did not experience any negative outcomes during their admission to be truly low risk.
Source: Coyne et al. Application of the MASCC and CISNE risk-stratification scores to identify low-risk febrile febrile neutropenic patients in the emergency department. Ann Emerg Med. 2017; 69(6): 755-764
For every patient, the authors calculated both the CISNE and MASCC scores to determine which was more accurate in identifying low-risk patients (See the Figure for details on how to calculate these scores). Ultimately, they found that the CISNE score was more accurate in identifying febrile neutropenic patients in the ED did not have an adverse event while hospitalized. The score was 100% specific in identifying all negative outcomes except for positive blood cultures for which the specificity was 97.4%. The positive predictive value of the CISNE score in the identification of low risk patients was found to be 98.1%. The MASCC score was less accurate at identifying low risk patients. The specificity for identifying low risk patients was only 54.2% and the positive predictive value was 84%.
This study provides evidence that the CISNE score can be used to accurately identify low-risk febrile neutropenic patients in the emergency department. The CISNE score was also found to be superior to the MASCC score. Although this study was a retrospective chart review, it provides evidence that the CISNE score may be helpful in determining which patients are at low risk of having adverse outcomes associated with their condition. There is growing evidence to suggest that these patients can be managed successfully as outpatients[4],[5]. Managing them as outpatients would not only save hospital resources but prevent exposing these patients to potentially harmful hospital acquired infections. While this paper is not enough justification to discharge these patients directly from the emergency department it does show that further research into this area is warranted and provides a potentially helpful risk stratification tool for emergency medicine physicians to help guide clinical decision making.
[1] Cooksley, T., Holland, M., and Klastersky, J. Ambulatory outpatient management of patients with low risk febrile neutropaenia. Acute Med. 2015; 14: 178–181
[2] Gea-Banacloche, J. Evidence-based approach to treatment of febrile neutropenia in hematologic malignancies. Hematol Am Soc Hematol Educ Program. 2013; 2013: 414–422
[3] Coyne C, Le V, Brennan J, Castillo E, Shatsky R, Ferran K, et al. Application of the MASCC and CISNE risk-stratification scores to identify low-risk febrile febrile neutropenic patients in the emergency department. Ann Emerg Med. 2017; 69(6): 755-764
[4] Flowers, C.R. and Karten, C. Communicating safe outpatient management of fever and neutropenia. J Oncol Pract. 2013; 9: 207–210
[5] Pherwani, N., Ghayad, J.M., Holle, L.M. et al. Outpatient management of febrile neutropenia associated with cancer chemotherapy: risk stratification and treatment review. Am J Health Syst Pharm. 2015; 72: 619–631
Greg Jasani is a fourth year medical student at the GW School of Medicine & Health Sciences
